
Page 118 - Read Online
P. 118
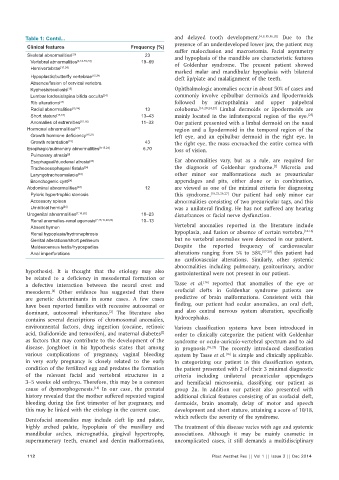
Table 1: Contd... and delayed tooth development. [4,9,15,16,20] Due to the
presence of an underdeveloped lower jaw, the patient may
Clinical features Frequency (%)
suffer malocclusion and macrostomia. Facial asymmetry
Skeletal abnormalities [20] 23 and hypoplasia of the mandible are characteristic features
Vertebral abnormalities [4,14-16,24] 19–69 of Goldenhar syndrome. The present patient showed
Hemivertebrae [15,24]
marked malar and mandibular hypoplasia with bilateral
Hypoplastic/butterfl y vertebrae [15,24] cleft lip/plate and malalignment of the teeth.
Absence/fusion of cervical vertebra
Kyphosis/scoliosis [15] Ophthalmologic anomalies occur in about 50% of cases and
Lumbar lordosis/spina bifi da occulta [24] commonly involve epibulbar dermoids and lipodermoids
Rib alterations [24] followed by micropthalmia and upper palpebral
Radial abnormalities [15,24] 13 coloboma. [16,20,24,25] Limbal dermoids or lipodermoids are
[25]
Short stature [15,16] 13–43 mainly located in the infratemporal region of the eye.
Anomalies of extremities [15,16] 11–33 Our patient presented with a limbal dermoid on the nasal
Hormonal abnormalities [21] region and a lipodermoid in the temporal region of the
Growth hormone defi ciency [15,21] left eye, and an epibulbar dermoid in the right eye. In
Growth retardation [15] 43 the right eye, the mass encroached the entire cornea with
Esophagic/pulmonary abnormalities [9,15,24] 6.70 loss of vision.
Pulmonary atresia [9]
Esophageal/duodenal atresia [24] Ear abnormalities vary, but as a rule, are required for
[7]
Tracheoesophageal fi stula [24] the diagnosis of Goldenhar syndrome. Microtia and
Laryngotracheomalacia [24] other minor ear malformations such as preauricular
Bronchogenic cyst [24] appendages and pits, either alone or in combination,
Abdominal abnormalities [20] 12 are viewed as one of the minimal criteria for diagnosing
Pyloric hypertrophic stenosis this syndrome. [18,23,26,27] Our patient had only minor ear
Accessory spleen abnormalities consisting of two preauricular tags, and this
Umbilical hernia [24] was a unilateral finding. He has not suffered any hearing
Urogenital abnormalities [7,16,20] 18–23 disturbances or facial nerve dysfunction.
Renal anomalies-renal agenesis [7,15,16,22,24] 10–13
Absent hymen Vertebral anomalies reported in the literature include
[14-16]
Renal hypoplasia/hydronephrosis hypoplasia, and fusion or absence of certain vertebra,
Genital alterations/short perineum but no vertebral anomalies were detected in our patient.
Maldescensus testis/hypospadias Despite the reported frequency of cardiovascular
Anal imperforations alterations ranging from 5% to 58%, [17-20] this patient had
no cardiovascular alterations. Similarly, other systemic
abnormalities including pulmonary, genitourinary, and/or
hypothesis). It is thought that the etiology may also gastrointestinal were not present in our patient.
be related to a deficiency in mesodermal formation or
[16]
a defective interaction between the neural crest and Tasse et al. reported that anomalies of the eye or
mesoderm. Other evidence has suggested that there orofacial clefts in Goldenhar syndrome patients are
[4]
are genetic determinants in some cases. A few cases predictive of brain malformations. Consistent with this
have been reported families with recessive autosomal or finding, our patient had ocular anomalies, an oral cleft,
dominant, autosomal inheritance. The literature also and also central nervous system alteration, specifically
[2]
contains several descriptions of chromosomal anomalies, hydrocephalus.
environmental factors, drug ingestion (cocaine, retinoic Various classification systems have been introduced in
acid, thalidomide and temoxifen), and maternal diabetes order to clinically categorize the patient with Goldenhar
[2]
as factors that may contribute to the development of the syndrome or oculo-auriculo-vertebral spectrum and to aid
disease. Jongbloet in his hypothesis states that among in prognosis. [16,25] The recently introduced classification
various complications of pregnancy, vaginal bleeding system by Tasse et al. is simple and clinically applicable.
[16]
in very early pregnancy is closely related to the early In categorizing our patient in this classification system,
condition of the fertilized egg and predates the formation the patient presented with 2 of their 3 minimal diagnostic
of the relevant facial and vertebral structures in a criteria including unilateral preauricular appendages
3–5 weeks old embryo. Therefore, this may be a common and hemifacial microsomia, classifying our patient as
cause of dysmorphogenesis. In our case, the prenatal group 2u. In addition our patient also presented with
[18]
history revealed that the mother suffered repeated vaginal additional clinical features consisting of an orofacial cleft,
bleeding during the first trimester of her pregnancy, and dermoids, brain anomaly, delay of motor and speech
this may be linked with the etiology in the current case. development and short stature, attaining a score of 10/18,
which reflects the severity of the syndrome.
Dentofacial anomalies may include cleft lip and palate,
highly arched palate, hypoplasia of the maxillary and The treatment of this disease varies with age and systemic
mandibular arches, micrognathia, gingival hypertrophy, associations. Although it may be mainly cosmetic in
supernumerary teeth, enamel and dentin malformations, uncomplicated cases, it still demands a multidisciplinary
112 Plast Aesthet Res || Vol 1 || Issue 3 || Dec 2014