
Page 487 - Read Online
P. 487
Smer et al. Mini-invasive Surg 2020;4:52 I http://dx.doi.org/10.20517/2574-1225.2020.36 Page 9 of 15
A B
C D
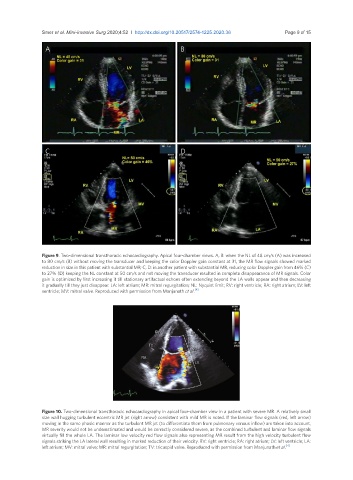
Figure 9. Two-dimensional transthoracic echocardiography. Apical four-chamber views. A, B: when the NL of 48 cm/s (A) was increased
to 80 cm/s (B) without moving the transducer and keeping the color Doppler gain constant at 31, the MR flow signals showed marked
reduction in size in this patient with substantial MR; C, D: in another patient with substantial MR, reducing color Doppler gain from 46% (C)
to 27% (D) keeping the NL constant at 50 cm/s and not moving the transducer resulted in complete disappearance of MR signals. Color
gain is optimized by first increasing it till stationary artifactual echoes often extending beyond the LA walls appear and then decreasing
it gradually till they just disappear. LA: left atrium; MR: mitral regurgitation; NL: Nyquist limit; RV: right ventricle; RA: right atrium; LV: left
[4]
ventricle; MV: mitral valve. Reproduced with permission from Manjunath et al.
Figure 10. Two-dimensional transthoracic echocardiography in apical four-chamber view in a patient with severe MR. A relatively small
size wall hugging turbulent eccentric MR jet (right arrow) consistent with mild MR is noted. If the laminar flow signals (red, left arrow)
moving in the same phasic manner as the turbulent MR jet (to differentiate them from pulmonary venous inflow) are taken into account,
MR severity would not be underestimated and would be correctly considered severe, as the combined turbulent and laminar flow signals
virtually fill the whole LA. The laminar low velocity red flow signals also representing MR result from the high velocity turbulent flow
signals striking the LA lateral wall resulting in marked reduction of their velocity. RV: right ventricle; RA: right atrium; LV: left ventricle; LA:
left atrium; MV: mitral valve; MR: mitral regurgitation; TV: tricuspid valve. Reproduced with permission from Manjunath et al. [4]