
Page 115 - Read Online
P. 115
Rao. Vessel Plus 2022;6:25 https://dx.doi.org/10.20517/2574-1209.2021.92 Page 25 of 41
Figure 43. Echo-Doppler studies in parasternal long (A) and short (B) axis and apical four-chamber (C) projections of the ventricular
septum demonstrating a small to moderate mid-muscular ventricular septal defect (VSD) with shunt from the left (LV) to the right
(RV) ventricle by color flow Doppler. Aorta (Ao) and left atrium (LA) are marked. Reproduced from Ref. [15] .
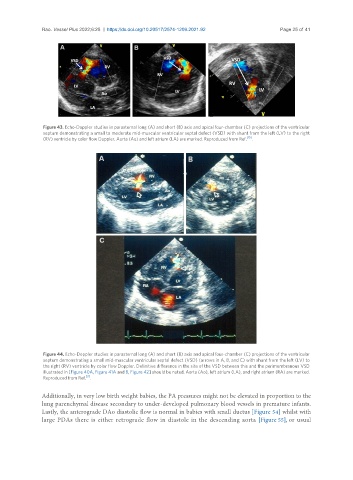
Figure 44. Echo-Doppler studies in parasternal long (A) and short (B) axis and apical four-chamber (C) projections of the ventricular
septum demonstrating a small mid-muscular ventricular septal defect (VSD) (arrows in A, B, and C) with shunt from the left (LV) to
the right (RV) ventricle by color flow Doppler. Definitive difference in the site of the VSD between this and the perimembranous VSD
illustrated in [Figure 40A, Figure 41A and B, Figure 42] should be noted. Aorta (Ao), left atrium (LA), and right atrium (RA) are marked.
[3]
Reproduced from Ref. .
Additionally, in very low birth weight babies, the PA pressures might not be elevated in proportion to the
lung parenchymal disease secondary to under-developed pulmonary blood vessels in premature infants.
Lastly, the anterograde DAo diastolic flow is normal in babies with small ductus [Figure 54] whilst with
large PDAs there is either retrograde flow in diastole in the descending aorta [Figure 55], or usual