
Page 113 - Read Online
P. 113
a b c
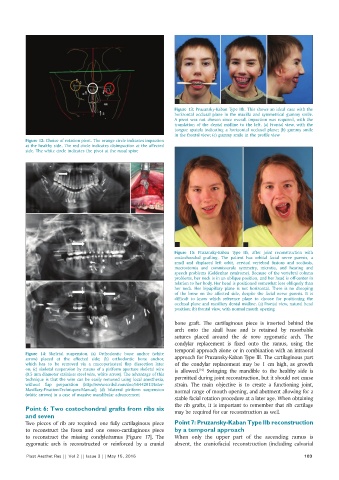
Figure 13: Pruzansky-Kaban Type IIb. This shows an ideal case with the
horizontal occlusal plane in the maxilla and symmetrical gummy smile.
A pivot was not chosen since overall impaction was required, with the
translation of the dental midline to the left. (a) Frontal view, with the
tongue spatula indicating a horizontal occlusal plane; (b) gummy smile
in the frontal view; (c) gummy smile in the profile view
Figure 12: Choice of rotation pivot. The orange circle indicates impaction
at the healthy side. The red circle indicates disimpaction at the affected
side. The white circle indicates the pivot at the nasal spine
a b
a b
Figure 15: Pruzansky-Kaban Type IIb, after joint reconstruction with
costochondral grafting. The patient has orbital facial nerve paresis, a
small and displaced left orbit, cervical vertebral fusions and scoliosis,
macrostomia and commissurala symmetry, microtia, and hearing and
speech problems (Goldenhar syndrome). Because of the vertebral column
c problems, her neck is in an oblique position, and her head is off-center in
relation to her body. Her head is positioned somewhat less obliquely than
her neck. Her bipupillary plane is not horizontal. There is no drooping
of the brow on the affected side, despite the facial nerve paresis. It is
difficult to know which reference plane to choose for positioning the
occlusal plane and maxillary dental midline. (a) Frontal view, natural head
position; (b) frontal view, with normal mouth opening
bone graft. The cartilaginous piece is inserted behind the
arch onto the skull base and is retained by resorbable
sutures placed around the de novo zygomatic arch. The
d condylar replacement is fixed onto the ramus, using the
Figure 14: Skeletal suspension. (a) Orthodontic bone anchor (white temporal approach alone or in combination with an intraoral
arrow) placed at the affected side; (b) orthodontic bone anchor, approach for Pruzansky-Kaban Type III. The cartilaginous part
which has to be removed via a mucoperiosteal flap dissection later of the condylar replacement may be 1 cm high, as growth
on; (c) skeletal suspension by means of a piriform aperture skeletal wire is allowed. Swinging the mandible to the healthy side is
[10]
(0.5 mm diameter stainless steel wire, white arrow). The advantage of this
technique is that the wire can be easily removed using local anesthesia, permitted during joint reconstruction, but it should not cause
without flap preparation (http://www.scribd.com/doc/56442013/Inter- strain. The main objective is to create a functioning joint,
Maxillary-Fixation-Techniques-Manual); (d) bilateral piriform suspension normal range of mouth opening, and abutment allowing for a
(white arrows) in a case of massive mandibular advancement
stable facial rotation procedure at a later age. When obtaining
the rib grafts, it is important to remember that rib cartilage
Point 6: Two costochondral grafts from ribs six may be required for ear reconstruction as well.
and seven
Two pieces of rib are required: one fully cartilaginous piece Point 7: Pruzansky‑Kaban Type IIb reconstruction
to reconstruct the fossa and one osseo-cartilaginous piece by a temporal approach
to reconstruct the missing condyle/ramus [Figure 17]. The When only the upper part of the ascending ramus is
zygomatic arch is reconstructed or reinforced by a cranial absent, the craniofacial reconstruction (including calvarial
Plast Aesthet Res || Vol 2 || Issue 3 || May 15, 2015 103