
Page 110 - Read Online
P. 110
a b
Figure 2: Ear deformities from 0 to 3 dysmorphic severity, as indicated
by the white arrow
c
Figure 1: An O0 M2a E2 N0 S2 case. (a) Frontal view; (b) left profile a b c
view; (c) frontal occlusion view
d e f
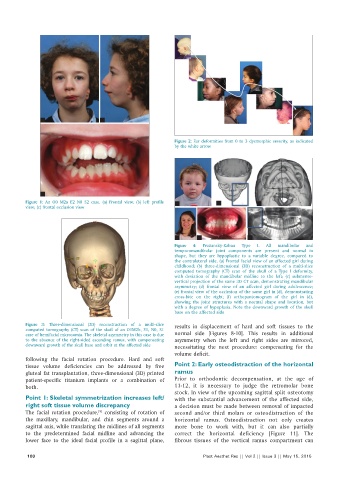
Figure 4: Pruzansky-Kaban Type I. All mandibular and
temporomandibular joint components are present and normal in
shape, but they are hypoplastic to a variable degree, compared to
the contralateral side. (a) Frontal facial view of an affected girl during
childhood; (b) three-dimensional (3D) reconstruction of a multi-slice
computed tomography (CT) scan of the skull of a Type I deformity,
with deviation of the mandibular midline to the left; (c) submento-
vertical projection of the same 3D CT scan, demonstrating mandibular
asymmetry; (d) frontal view of an affected girl during adolescence;
(e) frontal view of the occlusion of the same girl in (d), demonstrating
cross-bite on the right; (f) orthopantomogram of the girl in (d),
showing the joint structures with a normal shape and location, but
with a degree of hypoplasia. Note the downward growth of the skull
base on the affected side
Figure 3: Three-dimensional (3D) reconstruction of a multi-slice results in displacement of hard and soft tissues to the
computed tomography (CT) scan of the skull of an O1M2b, E1, N0, S1
case of hemifacial microsomia. The skeletal asymmetry in this case is due normal side [Figures 8-10]. This results in additional
to the absence of the right-sided ascending ramus, with compensating asymmetry when the left and right sides are mirrored,
downward growth of the skull base and orbit at the affected side necessitating the next procedure: compensating for the
volume deficit.
following the facial rotation procedure. Hard and soft
tissue volume deficiencies can be addressed by free Point 2: Early osteodistraction of the horizontal
gluteal fat transplantation, three-dimensional (3D) printed ramus
patient-specific titanium implants or a combination of Prior to orthodontic decompensation, at the age of
both. 11-12, it is necessary to judge the retromolar bone
stock. In view of the upcoming sagittal split osteotomy
Point 1: Skeletal symmetrization increases left/ with the substantial advancement of the affected side,
right soft tissue volume discrepancy a decision must be made between removal of impacted
The facial rotation procedure, consisting of rotation of second and/or third molars or osteodistraction of the
[9]
the maxillary, mandibular, and chin segments around a horizontal ramus. Osteodistraction not only creates
sagittal axis, while translating the midlines of all segments more bone to work with, but it can also partially
to the predetermined facial midline and advancing the correct the horizontal deficiency [Figure 11]. The
lower face to the ideal facial profile in a sagittal plane, fibrous tissues of the vertical ramus compartment can
100 Plast Aesthet Res || Vol 2 || Issue 3 || May 15, 2015