
Page 816 - Read Online
P. 816
Ancona et al. Mini-invasive Surg 2020;4:79 I http://dx.doi.org/10.20517/2574-1225.2020.80 Page 5 of 23
SGC
LA
SGC
LA
SGC
Ao
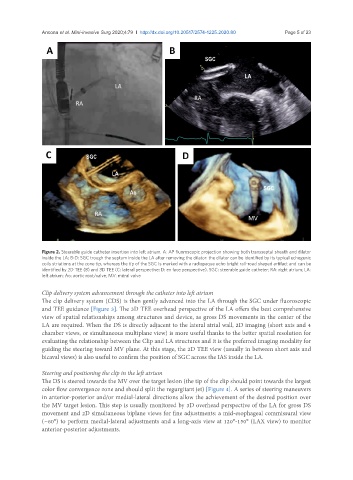
Figure 2. Steerable guide catheter insertion into left atrium. A: AP fluoroscopic projection showing both transseptal sheath and dilator
inside the LA; B-D: SGC trough the septum inside the LA after removing the dilator: the dilator can be identified by its typical echogenic
coils striations at the cone tip, whereas the tip of the SGC is marked with a radiopaque echo bright rail-road shaped artifact and can be
identified by 2D TEE (B) and 3D TEE (C: lateral perspective; D: en face perspective). SGC: steerable guide catheter; RA: right atrium; LA:
left atrium; Ao: aortic root/valve; MV: mitral valve
Clip delivery system advancement through the catheter into left atrium
The clip delivery system (CDS) is then gently advanced into the LA through the SGC under fluoroscopic
and TEE guidance [Figure 3]. The 3D TEE overhead perspective of the LA offers the best comprehensive
view of spatial relationships among structures and device, as gross DS movements in the center of the
LA are required. When the DS is directly adjacent to the lateral atrial wall, 2D imaging (short axis and 4
chamber views, or simultaneous multiplane view) is more useful thanks to the better spatial resolution for
evaluating the relationship between the Clip and LA structures and it is the preferred imaging modality for
guiding the steering toward MV plane. At this stage, the 2D TEE view (usually in between short axis and
bicaval views) is also useful to confirm the position of SGC across the IAS inside the LA.
Steering and positioning the clip in the left atrium
The DS is steered towards the MV over the target lesion (the tip of the clip should point towards the largest
color flow convergence zone and should split the regurgitant jet) [Figure 4]. A series of steering maneuvers
in anterior-posterior and/or medial-lateral directions allow the achievement of the desired position over
the MV target lesion. This step is usually monitored by 3D overhead perspective of the LA for gross DS
movement and 2D simultaneous biplane views for fine adjustments: a mid-esophageal commissural view
(~60°) to perform medial-lateral adjustments and a long-axis view at 120°-150° (LAX view) to monitor
anterior-posterior adjustments.