
Page 21 - Read Online
P. 21
Castán et al. Radiology of hepatocarcinoma in non-cirrhotic patients
A B C
D E F
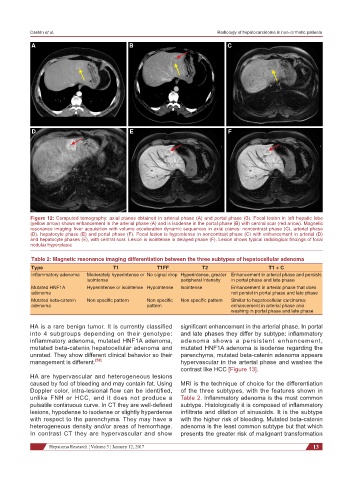
Figure 12: Computed tomography: axial planes obtained in arterial phase (A) and portal phase (B). Focal lesion in left hepatic lobe
(yellow arrow) shows enhancement in the arterial phase (A) and is isodense in the portal phase (B) with central scar (red arrow). Magnetic
resonance imaging: liver acquisition with volume acceleration dynamic sequences in axial planes: noncontrast phase (C), arterial phase
(D), hepatocyte phase (E) and portal phase (F). Focal lesion is hypointense in noncontrast phase (C) with enhancement in arterial (D)
and hepatocyte phases (E), with central scar. Lesion is isointense in delayed phase (F). Lesion shows typical radiological findings of focal
nodular hyperplasia
Table 2: Magnetic resonance imaging differentiation between the three subtypes of hepatocellular adenoma
Type T1 T1FF T2 T1 + C
Inflammatory adenoma Moderately hyperintense or No signal drop Hyperintense, greater Enhancement in arterial phase and persists
isointense peripheral intensity in portal phase and late phase
Mutated HNF1A Hyperintense or isointense Hypointense Isointense Enhancement in arterial phase that does
adenoma not persist in portal phase and late phase
Mutated beta-catenin Non specific pattern Non specific Non specific pattern Similar to hepatocellular carcinoma:
adenoma pattern enhancement in arterial phase and
washing in portal phase and late phase
HA is a rare benign tumor. It is currently classified significant enhancement in the arterial phase. In portal
into 4 subgroups depending on their genotype: and late phases they differ by subtype: inflammatory
inflammatory adenoma, mutated HNF1A adenoma, adenoma shows a persistent enhancement,
mutated beta-catenin hepatocellular adenoma and mutated HNF1A adenoma is isodense regarding the
unrated. They show different clinical behavior so their parenchyma, mutated beta-catenin adenoma appears
management is different. [53] hypervascular in the arterial phase and washes the
contrast like HCC [Figure 13].
HA are hypervascular and heterogeneous lesions
caused by foci of bleeding and may contain fat. Using MRI is the technique of choice for the differentiation
Doppler color, intra-lesional flow can be identified, of the three subtypes, with the features shown in
unlike FNH or HCC, and it does not produce a Table 2. Inflammatory adenoma is the most common
pulsatile continuous curve. In CT they are well-defined subtype. Histologically it is composed of inflammatory
lesions, hypodense to isodense or slightly hyperdense infiltrate and dilation of sinusoids. It is the subtype
with respect to the parenchyma. They may have a with the higher risk of bleeding. Mutated beta-catenin
heterogeneous density and/or areas of hemorrhage. adenoma is the least common subtype but that which
In contrast CT they are hypervascular and show presents the greater risk of malignant transformation
Hepatoma Research ¦ Volume 3 ¦ January 12, 2017 13