
Page 213 - Read Online
P. 213
Page 14 of 23 Farber et al. Plast Aesthet Res 2020;7:20 I http://dx.doi.org/10.20517/2347-9264.2020.05
A
B
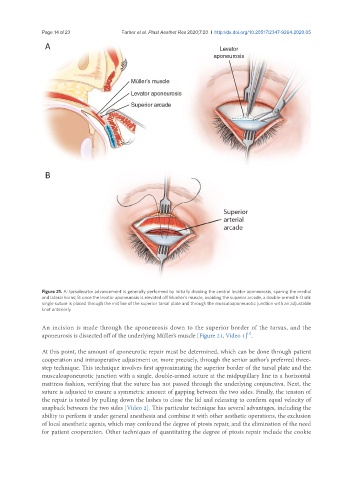
Figure 21. A: tarsolevator advancement is generally performed by initially dividing the central levator aponeurosis, sparing the medial
and lateral horns; B: once the levator aponeurosis is elevated off Mueller’s muscle, avoiding the superior arcade, a double-armed 6-0 silk
single suture is placed through the midline of the superior tarsal plate and through the musculoaponeurotic junction with an adjustable
knot anteriorly
An incision is made through the aponeurosis down to the superior border of the tarsus, and the
[1]
aponeurosis is dissected off of the underlying Müller’s muscle [Figure 21, Video 1] .
At this point, the amount of aponeurotic repair must be determined, which can be done through patient
cooperation and intraoperative adjustment or, more precisely, through the senior author’s preferred three-
step technique. This technique involves first approximating the superior border of the tarsal plate and the
musculoaponeurotic junction with a single, double-armed suture at the midpupillary line in a horizontal
mattress fashion, verifying that the suture has not passed through the underlying conjunctiva. Next, the
suture is adjusted to ensure a symmetric amount of gapping between the two sides. Finally, the tension of
the repair is tested by pulling down the lashes to close the lid and releasing to confirm equal velocity of
snapback between the two sides [Video 2]. This particular technique has several advantages, including the
ability to perform it under general anesthesia and combine it with other aesthetic operations, the exclusion
of local anesthetic agents, which may confound the degree of ptosis repair, and the elimination of the need
for patient cooperation. Other techniques of quantitating the degree of ptosis repair include the cookie