
Page 212 - Read Online
P. 212
Farber et al. Plast Aesthet Res 2020;7:20 I http://dx.doi.org/10.20517/2347-9264.2020.05 Page 13 of 23
Figure 19. The approximate skin markings for tarsolevator advancement uses an anterior approach similar to an upper blepharoplasty
A B
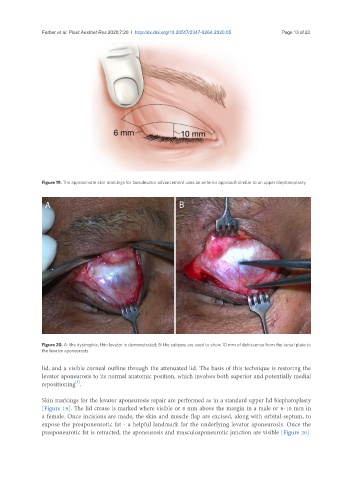
Figure 20. A: the dystrophic, thin levator is demonstrated; B: the calipers are used to show 10 mm of dehiscence from the tarsal plate to
the levator aponeurosis
lid, and a visible corneal outline through the attenuated lid. The basis of this technique is restoring the
levator aponeurosis to its normal anatomic position, which involves both superior and potentially medial
[1]
repositioning .
Skin markings for the levator aponeurosis repair are performed as in a standard upper lid blepharoplasty
[Figure 19]. The lid crease is marked where visible or 8 mm above the margin in a male or 8-10 mm in
a female. Once incisions are made, the skin and muscle flap are excised, along with orbital septum, to
expose the preaponeurotic fat - a helpful landmark for the underlying levator aponeurosis. Once the
preaponeurotic fat is retracted, the aponeurosis and musculoaponeurotic junction are visible [Figure 20].