
Page 14 - Read Online
P. 14
Deldar et al. Plast Aesthet Res 2022;9:13 https://dx.doi.org/10.20517/2347-9264.2021.100 Page 7 of 16
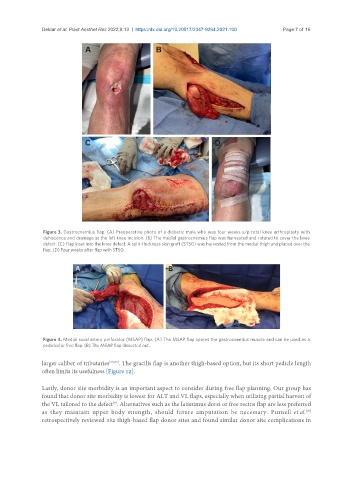
Figure 3. Gastrocnemius flap. (A) Preoperative photo of a diabetic male who was four weeks s/p total knee arthroplasty with
dehiscence and drainage at the left knee incision. (B) The medial gastrocnemius flap was harvested and rotated to cover the knee
defect. (C) Flap inset into the knee defect. A split-thickness skin graft (STSG) was harvested from the medial thigh and placed over the
flap. (D) Four weeks after flap with STSG.
Figure 4. Medial sural artery perforator (MSAP) flap. (A) The MSAP flap spares the gastrocnemius muscle and can be used as a
pedicled or free flap. (B) The MSAP flap dissected out.
larger caliber of tributaries [65,69] . The gracilis flap is another thigh-based option, but its short pedicle length
often limits its usefulness [Figure 12].
Lastly, donor site morbidity is an important aspect to consider during free flap planning. Our group has
found that donor site morbidity is lowest for ALT and VL flaps, especially when utilizing partial harvest of
the VL tailored to the defect . Alternatives such as the latissimus dorsi or free rectus flap are less preferred
[9]
as they maintain upper body strength, should future amputation be necessary. Purnell et al.
[70]
retrospectively reviewed 352 thigh-based flap donor sites and found similar donor site complications in