
Page 61 - Read Online
P. 61
Griffiths et al. Neuroimmunol Neuroinflammation 2020;7:51-67 I http://dx.doi.org/10.20517/2347-8659.2019.21 Page 57
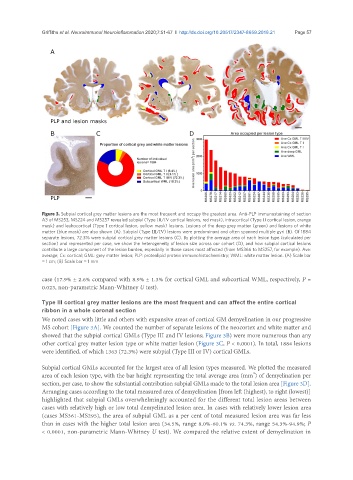
Figure 3. Subpial cortical grey matter lesions are the most frequent and occupy the greatest area. Anti-PLP immunostaining of section
A3 of MS253, MS224 and MS257 revealed subpial (Type III/IV cortical lesions, red mask), intracortical (Type II cortical lesion, orange
mask) and leukocortical (Type I cortical lesion, yellow mask) lesions. Lesions of the deep grey matter (green) and lesions of white
matter (blue mask) are also shown (A). Subpial (Type III/IV) lesions were predominant and often spanned multiple gyri (B). Of 1884
separate lesions, 72.3% were subpial cortical grey matter lesions (C). By plotting the average area of each lesion type (calculated per
section) and represented per case, we show the heterogeneity of lesion size across our cohort (D), and how subpial cortical lesions
contribute a large component of the lesion burden, especially in those cases most affected (from MS366 to MS257, for example). Ave:
average; Cx: cortical; GML: grey matter lesion; PLP: proteolipid protein immunohistochemistry; WML: white matter lesion. (A) Scale bar
= 1 cm; (B) Scale bar = 1 mm
case (17.9% ± 2.6% compared with 8.9% ± 1.3% for cortical GML and subcortical WML, respectively, P =
0.023, non-parametric Mann-Whitney U test).
Type III cortical grey matter lesions are the most frequent and can affect the entire cortical
ribbon in a whole coronal section
We noted cases with little and others with expansive areas of cortical GM demyelination in our progressive
MS cohort [Figure 3A]. We counted the number of separate lesions of the neocortex and white matter and
showed that the subpial cortical GMLs (Type III and IV lesions; Figure 3B) were more numerous than any
other cortical grey matter lesion type or white matter lesion (Figure 3C, P < 0.0001). In total, 1884 lesions
were identified, of which 1363 (72.3%) were subpial (Type III or IV) cortical GMLs.
Subpial cortical GMLs accounted for the largest area of all lesion types measured. We plotted the measured
2
area of each lesion type, with the bar height representing the total average area (mm ) of demyelination per
section, per case, to show the substantial contribution subpial GMLs made to the total lesion area [Figure 3D].
Arranging cases according to the total measured area of demyelination [from left (highest), to right (lowest)]
highlighted that subpial GMLs overwhelmingly accounted for the different total lesion areas between
cases with relatively high or low total demyelinated lesion area. In cases with relatively lower lesion area
(cases MS361-MS295), the area of subpial GML as a per cent of total measured lesion area was far less
than in cases with the higher total lesion area (34.5%, range 8.0%-60.1% vs. 74.3%, range 54.3%-94.9%; P
< 0.0001, non-parametric Mann-Whitney U test). We compared the relative extent of demyelination in