
Page 130 - Read Online
P. 130
was firm in consistency and very vascular in nature but and large atypical cells with prominent nuclei and
eventually we were able to achieve gross total resection. nucleoli [Figure 4a]. Abnormal mitotic figures and
The early postoperative course was unremarkable for apoptotic nuclei were common. The tight collections of
any neurological deficits until patient deteriorated neoplastic cells were surrounded by rich fibrovascular
few hours thereafter and had asymmetric blown stroma forming the architectural patterns of “Zellballen”.
pupils. Owing to the urgency of the case, the patient The majority of the neoplastic cells were strongly
was taken for surgery with a provisional diagnosis of positive for chromogranin, synaptophysin (SYN),
postoperative bleeding. Surgical re-exploration was and neuron-specific enolase, and focally for tyrosine
done, and large intracerebral hematoma within the hydroxylase [Figure 4b]. Ganglionic cells displayed
tumor bed was evacuated. The patient, unfortunately, strong cytoplasmic reaction for SYN and less often
woke up postoperatively with dense left sided tubulin [Figure 4c]. Glial fibrillary acidic protein showed
hemiplegia [Figure 3]. very strong reaction in the cells outlining the edges of the
neoplastic congregates, in a pattern seen in sustentacular
Microscopic examination of the tumor revealed cells of extracranial paragangliomas [Figure 4d]. The
nests of highly pleomorphic, spindle, epithelioid, rest of the immunohistochemistry is outlined in Table 1.
At this point, an extensive metastatic work up had
been done which included CT of her chest, abdomen,
and pelvis, as well as mammogram. Due to the fact
that this tumor has been frequently originating from
the duodenum, a duodenal scope was also performed.
The analysis resulted negative for any primary lesions.
As some paragangliomas can be functionally active,
serum and urine metanephrines, and catecholamines
were investigated and resulted also negative. Given
these results and the pathological features of the
resected tumor, the assumption was made being a
primary malignant gangliocytic paraganglioma. The
patient was approached in a multidisciplinary team
including the radiation oncology and offered local
Figure 1: Preoperative plain computed tomography head shows a right-sided
isodense lesion within the insular region tumor bed radiation. Due to low karnofsky performance
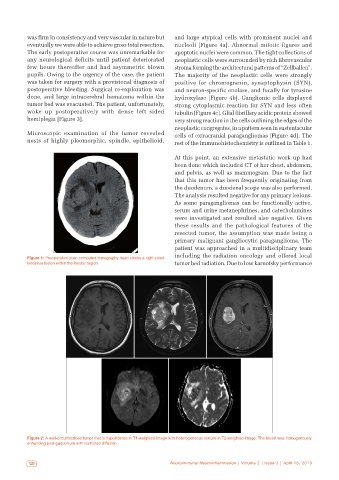
Figure 2: A well-circumscribed tumor that is hypointense in T1-weighted image with heterogeneous texture in T2-weighted image. The lesion was homogenously
enhancing post-gadolinium with restricted diffusion
122 Neuroimmunol Neuroinflammation | Volume 2 | Issue 2 | April 15, 2015