
Page 575 - Read Online
P. 575
Cossu et al. Mini-invasive Surg 2020;4:60 I http://dx.doi.org/10.20517/2574-1225.2020.52 Page 7 of 15
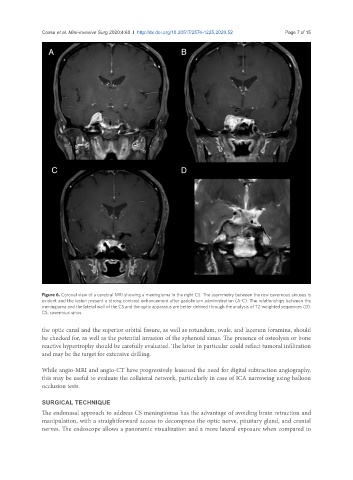
Figure 6. Coronal view of a cerebral MRI showing a meningioma in the right CS. The asymmetry between the row cavernous sinuses is
evident and the lesion present a strong contrast enhancement after gadolinium administration (A-C). The relationships between the
meningioma and the lateral wall of the CS and the optic apparatus are better defined through the analysis of T2-weighted sequences (D).
CS: cavernous sinus
the optic canal and the superior orbital fissure, as well as rotundum, ovale, and lacerum foramina, should
be checked for, as well as the potential invasion of the sphenoid sinus. The presence of osteolysis or bone
reactive hypertrophy should be carefully evaluated. The latter in particular could reflect tumoral infiltration
and may be the target for extensive drilling.
While angio-MRI and angio-CT have progressively lessened the need for digital subtraction angiography,
this may be useful to evaluate the collateral network, particularly in case of ICA narrowing using balloon
occlusion tests.
SURGICAL TECHNIQUE
The endonasal approach to address CS meningiomas has the advantage of avoiding brain retraction and
manipulation, with a straightforward access to decompress the optic nerve, pituitary gland, and cranial
nerves. The endoscope allows a panoramic visualization and a more lateral exposure when compared to