
Page 573 - Read Online
P. 573
Cossu et al. Mini-invasive Surg 2020;4:60 I http://dx.doi.org/10.20517/2574-1225.2020.52 Page 5 of 15
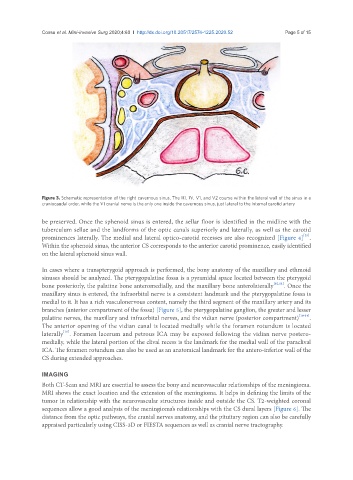
Figure 3. Schematic representation of the right cavernous sinus. The III, IV, V1, and V2 course within the lateral wall of the sinus in a
craniocaudal order, while the VI cranial nerve is the only one inside the cavernous sinus, just lateral to the internal carotid artery
be preserved. Once the sphenoid sinus is entered, the sellar floor is identified in the midline with the
tuberculum sellae and the landforms of the optic canals superiorly and laterally, as well as the carotid
[25]
prominences laterally. The medial and lateral optico-carotid recesses are also recognized [Figure 4] .
Within the sphenoid sinus, the anterior CS corresponds to the anterior carotid prominence, easily identified
on the lateral sphenoid sinus wall.
In cases where a transpterygoid approach is performed, the bony anatomy of the maxillary and ethmoid
sinuses should be analyzed. The pterygopalatine fossa is a pyramidal space located between the pterygoid
bone posteriorly, the palatine bone anteromedially, and the maxillary bone anterolaterally [10,11] . Once the
maxillary sinus is entered, the infraorbital nerve is a consistent landmark and the pterygopalatine fossa is
medial to it. It has a rich vasculonervous content, namely the third segment of the maxillary artery and its
branches (anterior compartment of the fossa) [Figure 5], the pterygopalatine ganglion, the greater and lesser
palatine nerves, the maxillary and infraorbital nerves, and the vidian nerve (posterior compartment) [10-14] .
The anterior opening of the vidian canal is located medially while the foramen rotundum is located
[10]
laterally . Foramen lacerum and petrous ICA may be exposed following the vidian nerve postero-
medially, while the lateral portion of the clival recess is the landmark for the medial wall of the paraclival
ICA. The foramen rotundum can also be used as an anatomical landmark for the antero-inferior wall of the
CS during extended approaches.
IMAGING
Both CT-Scan and MRI are essential to assess the bony and neurovascular relationships of the meningioma.
MRI shows the exact location and the extension of the meningioma. It helps in defining the limits of the
tumor in relationship with the neurovascular structures inside and outside the CS. T2-weighted coronal
sequences allow a good analysis of the meningioma’s relationships with the CS dural layers [Figure 6]. The
distance from the optic pathways, the cranial nerves anatomy, and the pituitary region can also be carefully
appraised particularly using CISS-3D or FIESTA sequences as well as cranial nerve tractography.