
Page 81 - Read Online
P. 81
Tropiano et al. Mini-invasive Surg 2024;8:17 https://dx.doi.org/10.20517/2574-1225.2024.41 Page 11 of 15
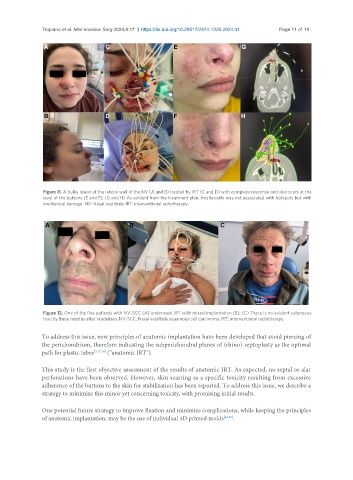
Figure 11. A bulky lesion of the lateral wall of the NV (A and B) treated by IRT (C and D) with complete response and skin scars at the
level of the buttons (E and F); (G and H) As evident from the treatment plan, this toxicity was not associated with hotspots but with
mechanical damage. NV: Nasal vestibule; IRT: interventional radiotherapy.
Figure 12. One of the five patients with NV-SCC (A) underwent IRT with mixed implantation (B); (C) There is no evident cutaneous
toxicity three months after irradiation. NV-SCC: Nasal vestibule squamous cell carcinoma; IRT: interventional radiotherapy.
To address this issue, new principles of anatomic implantation have been developed that avoid piercing of
the perichondrium, therefore indicating the subperichondral planes of (rhino)-septoplasty as the optimal
path for plastic tubes [3,17,18] (“anatomic IRT”).
This study is the first objective assessment of the results of anatomic IRT. As expected, no septal or alar
perforations have been observed. However, skin scarring as a specific toxicity resulting from excessive
adherence of the buttons to the skin for stabilization has been reported. To address this issue, we describe a
strategy to minimize this minor yet concerning toxicity, with promising initial results.
One potential future strategy to improve fixation and minimize complications, while keeping the principles
of anatomic implantation, may be the use of individual 3D printed molds [46,47] .