
Page 75 - Read Online
P. 75
Tropiano et al. Mini-invasive Surg 2024;8:17 https://dx.doi.org/10.20517/2574-1225.2024.41 Page 5 of 15
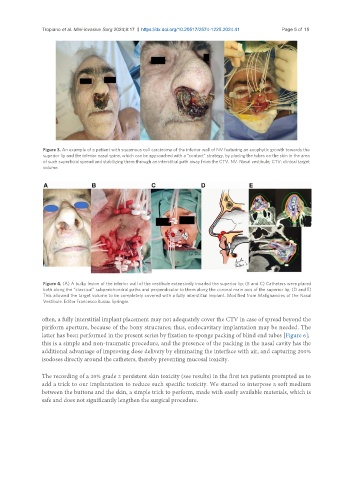
Figure 3. An example of a patient with squamous cell carcinoma of the inferior wall of NV featuring an exophytic growth towards the
superior lip and the inferior nasal spine, which can be approached with a “contact” strategy, by placing the tubes on the skin in the area
of such superficial spread and stabilizing them through an interstitial path away from the CTV. NV: Nasal vestibule; CTV: clinical target
volume.
Figure 4. (A) A bulky lesion of the inferior wall of the vestibule extensively invaded the superior lip; (B and C) Catheters were placed
both along the “classical” subperichondral paths and perpendicular to them along the coronal main axis of the superior lip; (D and E)
This allowed the target volume to be completely covered with a fully interstitial implant. Modified from Malignancies of the Nasal
Vestibule. Editor Francesco Bussu. Springer.
often, a fully interstitial implant placement may not adequately cover the CTV in case of spread beyond the
piriform aperture, because of the bony structures; thus, endocavitary implantation may be needed. The
latter has been performed in the present series by fixation to sponge packing of blind end tubes [Figure 6];
this is a simple and non-traumatic procedure, and the presence of the packing in the nasal cavity has the
additional advantage of improving dose delivery by eliminating the interface with air, and capturing 200%
isodoses directly around the catheters, thereby preventing mucosal toxicity.
The recording of a 20% grade 2 persistent skin toxicity (see results) in the first ten patients prompted us to
add a trick to our implantation to reduce such specific toxicity. We started to interpose a soft medium
between the buttons and the skin, a simple trick to perform, made with easily available materials, which is
safe and does not significantly lengthen the surgical procedure.