
Page 236 - Read Online
P. 236
Page 12 of 20 Siegal et al. Plast Aesthet Res 2019;6:25 I http://dx.doi.org/10.20517/2347-9264.2019.35
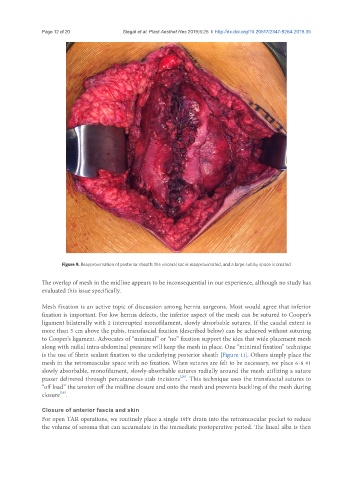
Figure 9. Reapproximation of posterior sheath: the visceral sac is reapproximated, and a large sublay space is created
The overlap of mesh in the midline appears to be inconsequential in our experience, although no study has
evaluated this issue specifically.
Mesh fixation is an active topic of discussion among hernia surgeons. Most would agree that inferior
fixation is important. For low hernia defects, the inferior aspect of the mesh can be sutured to Cooper’s
ligament bilaterally with 2 interrupted monofilament, slowly absorbable sutures. If the caudal extent is
more than 5 cm above the pubis, transfascial fixation (described below) can be achieved without suturing
to Cooper’s ligament. Advocates of “minimal” or “no” fixation support the idea that wide placement mesh
along with radial intra-abdominal pressure will keep the mesh in place. One “minimal fixation” technique
is the use of fibrin sealant fixation to the underlying posterior sheath [Figure 11]. Others simply place the
mesh in the retromuscular space with no fixation. When sutures are felt to be necessary, we place 6-8 #1
slowly absorbable, monofilament, slowly-absorbable sutures radially around the mesh utilizing a suture
[28]
passer delivered through percutaneous stab incisions . This technique uses the transfascial sutures to
“off load” the tension off the midline closure and onto the mesh and prevents buckling of the mesh during
[29]
closure .
Closure of anterior fascia and skin
For open TAR operations, we routinely place a single 19Fr drain into the retromuscular pocket to reduce
the volume of seroma that can accumulate in the immediate postoperative period. The lineal alba is then