
Page 237 - Read Online
P. 237
Siegal et al. Plast Aesthet Res 2019;6:25 I http://dx.doi.org/10.20517/2347-9264.2019.35 Page 13 of 20
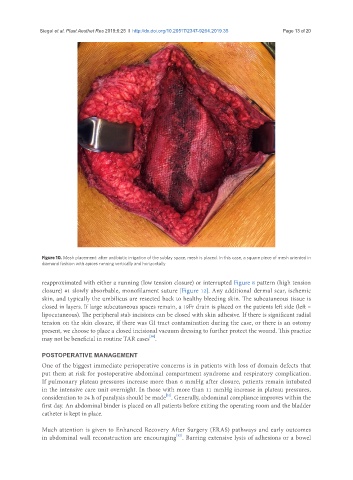
Figure 10. Mesh placement: after antibiotic irrigation of the sublay space, mesh is placed. In this case, a square piece of mesh oriented in
diamond fashion with apices running vertically and horizontally
reapproximated with either a running (low tension closure) or interrupted Figure 8 pattern (high tension
closure) #1 slowly absorbable, monofilament suture [Figure 12]. Any additional dermal scar, ischemic
skin, and typically the umbilicus are resected back to healthy bleeding skin. The subcutaneous tissue is
closed in layers. If large subcutaneous spaces remain, a 19Fr drain is placed on the patients left side (left =
lipocutaneous). The peripheral stab incisions can be closed with skin adhesive. If there is significant radial
tension on the skin closure, if there was GI tract contamination during the case, or there is an ostomy
present, we choose to place a closed incisional vacuum dressing to further protect the wound. This practice
[30]
may not be beneficial in routine TAR cases .
POSTOPERATIVE MANAGEMENT
One of the biggest immediate perioperative concerns is in patients with loss of domain defects that
put them at risk for postoperative abdominal compartment syndrome and respiratory complication.
If pulmonary plateau pressures increase more than 6 mmHg after closure, patients remain intubated
in the intensive care unit overnight. In those with more than 11 mmHg increase in plateau pressures,
[31]
consideration to 24 h of paralysis should be made . Generally, abdominal compliance improves within the
first day. An abdominal binder is placed on all patients before exiting the operating room and the bladder
catheter is kept in place.
Much attention is given to Enhanced Recovery After Surgery (ERAS) pathways and early outcomes
[32]
in abdominal wall reconstruction are encouraging . Barring extensive lysis of adhesions or a bowel