
Page 238 - Read Online
P. 238
Page 14 of 20 Siegal et al. Plast Aesthet Res 2019;6:25 I http://dx.doi.org/10.20517/2347-9264.2019.35
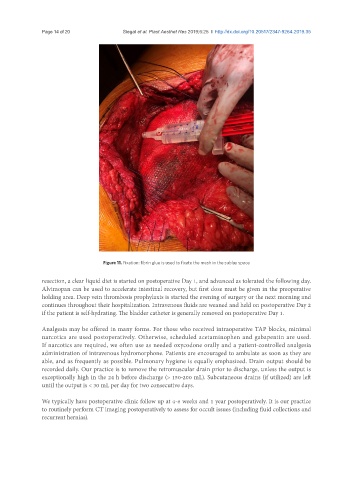
Figure 11. Fixation: fibrin glue is used to fixate the mesh in the sublay space
resection, a clear liquid diet is started on postoperative Day 1, and advanced as tolerated the following day.
Alvimopan can be used to accelerate intestinal recovery, but first dose must be given in the preoperative
holding area. Deep vein thrombosis prophylaxis is started the evening of surgery or the next morning and
continues throughout their hospitalization. Intravenous fluids are weaned and held on postoperative Day 2
if the patient is self-hydrating. The bladder catheter is generally removed on postoperative Day 1.
Analgesia may be offered in many forms. For those who received intraoperative TAP blocks, minimal
narcotics are used postoperatively. Otherwise, scheduled acetaminophen and gabapentin are used.
If narcotics are required, we often use as needed oxycodone orally and a patient-controlled analgesia
administration of intravenous hydromorphone. Patients are encouraged to ambulate as soon as they are
able, and as frequently as possible. Pulmonary hygiene is equally emphasized. Drain output should be
recorded daily. Our practice is to remove the retromuscular drain prior to discharge, unless the output is
exceptionally high in the 24 h before discharge (> 150-200 mL). Subcutaneous drains (if utilized) are left
until the output is < 30 mL per day for two consecutive days.
We typically have postoperative clinic follow up at 4-6 weeks and 1 year postoperatively. It is our practice
to routinely perform CT imaging postoperatively to assess for occult issues (including fluid collections and
recurrent hernias).