
Page 310 - Read Online
P. 310
Rosen et al. Barbed vs. smooth suture for periareolar closure
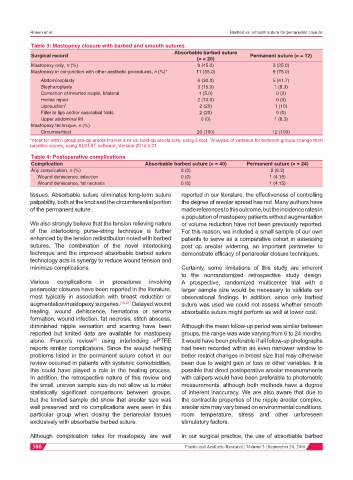
Table 3: Mastopexy closure with barbed and smooth sutures
Absorbable barbed suture
Surgical record Permanent suture (n = 12)
(n = 20)
Mastopexy only, n (%) 9 (45.0) 3 (25.0)
Mastopexy in conjunction with other aesthetic procedures, n (%)* 11 (55.0) 9 (75.0)
Abdominoplasty 6 (30.0) 5 (41.7)
Blepharoplasty 3 (15.0) 1 (8.3)
Correction of inverted nipple, bilateral 1 (5.0) 0 (0)
Hernia repair 2 (10.0) 0 (0)
Liposuction † 2 (20) 1 (10)
Filler to lips and/or nasolabial folds 2 (20) 0 (0)
Upper abdominal lift 0 (0) 1 (8.3)
Mastopexy technique, n (%)
Circumvertical 20 (100) 12 (100)
*t-test for within group pre-op areola marker size vs. post-op areola size, using Excel. Analysis of variance for between groups change from
†
baseline scores, using XLSTAT software, Version 2014.5.01
Table 4: Postoperative complications
Complication Absorbable barbed suture (n = 40) Permanent suture (n = 24)
Any complication, n (%) 0 (0) 2 (8.3)
Wound dehiscence, infection 0 (0) 1 (4.15)
Wound dehiscence, fat necrosis 0 (0) 1 (4.15)
tissues. Absorbable suture eliminates long-term suture reported in our literature, the effectiveness of controlling
palpability, both at the knot and the circumferential portion the degree of areolar spread has not. Many authors have
of the permanent suture. made references to this outcome, but the incidence rates in
a population of mastopexy patients without augmentation
We also strongly believe that the tension relieving nature or volume reduction have not been previously reported.
of the interlocking purse-string technique is further For this reason, we included a small sample of our own
enhanced by the tension redistribution noted with barbed patients to serve as a comparative cohort in assessing
sutures. The combination of the novel interlocking post op areolar widening, an important parameter to
technique and the improved absorbable barbed suture demonstrate efficacy of periareolar closure techniques.
technology acts in synergy to reduce wound tension and
minimize complications. Certainly, some limitations of this study are inherent
to the nonrandomized retrospective study design.
Various complications in procedures involving A prospective, randomized multicenter trial with a
periareolar closures have been reported in the literature, larger sample size would be necessary to validate our
most typically in association with breast reduction or observational findings. In addition, since only barbed
augmentation/mastopexy surgeries. [16-21] Delayed wound suture was used we could not assess whether smooth
healing, wound dehiscence, hematoma or seroma absorbable suture might perform as well at lower cost.
formation, wound infection, fat necrosis, stitch abscess,
diminished nipple sensation and scarring have been Although the mean follow-up period was similar between
reported but limited data are available for mastopexy groups, the range was wide varying from 6 to 24 months.
alone. Franco’s review using interlocking ePTFE It would have been preferable if all follow-up photographs
[6]
reports similar complications. Since the wound healing had been recorded within an even narrower window to
problems listed in the permanent suture cohort in our better restrict changes in breast size that may otherwise
review occurred in patients with systemic comorbidities, been due to weight gain or loss or other variables. It is
this could have played a role in the healing process. possible that direct postoperative areolar measurements
In addition, the retrospective nature of this review and with calipers would have been preferable to photometric
the small, uneven sample size do not allow us to make measurements, although both methods have a degree
statistically significant comparisons between groups, of inherent inaccuracy. We are also aware that due to
but the limited sample did show that areolar size was the contractile properties of the nipple areolar complex,
well preserved and no complications were seen in this areolar size may vary based on environmental conditions,
particular group when closing the periareolar tissues room temperature, stress and other unforeseen
exclusively with absorbable barbed suture. stimulatory factors.
Although complication rates for mastopexy are well In our surgical practice, the use of absorbable barbed
300 Plastic and Aesthetic Research ¦ Volume 3 ¦ September 20, 2016