
Page 304 - Read Online
P. 304
Hwang et al. Medially based de-epithelialized flap
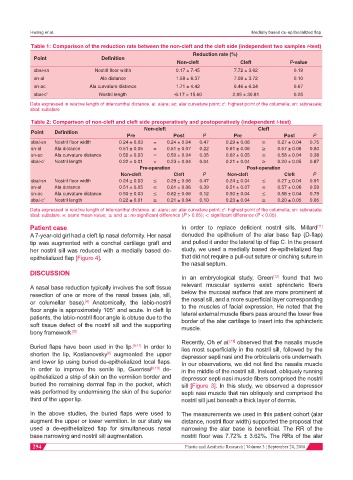
Table 1: Comparison of the reduction rate between the non-cleft and the cleft side (independent two samples t-test)
Reduction rate (%)
Point Definition
Non-cleft Cleft P-value
sbal-sn Nostril floor width 0.17 ± 7.45 7.72 ± 3.62 0.19
sn-al Ala distance 1.58 ± 6.37 7.09 ± 3.72 0.10
sn-ac Ala curvature distance 1.71 ± 4.42 6.46 ± 6.24 0.67
sbal-c’ Nostril length -6.17 ± 15.60 2.95 ± 30.81 0.25
Data expressed in relative length of intercanthal distance. al: alare; ac: alar curvature point; c’: highest point of the columella; sn: subnasale;
sbal: subalare
Table 2: Comparison of non-cleft and cleft side preoperatively and postoperatively (independent t-test)
Non-cleft Cleft
Point Definition
Pre Post P Pre Post P
sbal-sn Nostril floor width 0.24 ± 0.03 = 0.24 ± 0.04 0.47 0.29 ± 0.06 ≥ 0.27 ± 0.04 0.75
sn-al Ala distance 0.51 ± 0.05 = 0.51 ± 0.07 0.22 0.61 ± 0.06 ≥ 0.57 ± 0.06 0.80
sn-ac Ala curvature distance 0.50 ± 0.03 = 0.50 ± 0.04 0.35 0.62 ± 0.05 ≥ 0.58 ± 0.04 0.38
sbal-c’ Nostril length 0.22 ± 0.01 < 0.23 ± 0.04 0.04 0.21 ± 0.04 ≥ 0.20 ± 0.05 0.87
Pre-operation Post-operation
Non-cleft Cleft P Non-cleft Cleft P
sbal-sn Nostril floor width 0.24 ± 0.03 ≤ 0.29 ± 0.06 0.47 0.24 ± 0.04 ≤ 0.27 ± 0.04 0.91
sn-al Ala distance 0.51 ± 0.05 ≤ 0.61 ± 0.06 0.39 0.51 ± 0.07 ≤ 0.57 ± 0.06 0.59
sn-ac Ala curvature distance 0.50 ± 0.03 ≤ 0.62 ± 0.06 0.12 0.50 ± 0.04 ≤ 0.58 ± 0.04 0.79
sbal-c’ Nostril length 0.22 ± 0.01 ≥ 0.21 ± 0.04 0.10 0.23 ± 0.04 ≥ 0.20 ± 0.05 0.85
Data expressed in relative length of intercanthal distance. al: alare; ac: alar curvature point; c’: highest point of the columella; sn: subnasale;
sbal: subalare. =: same mean value; ≥ and ≤: no significant difference (P > 0.05); <: significant difference (P < 0.05)
Patient case In order to replace deficient nostril sills, Millard
[11]
A 7-year-old girl had a cleft lip nasal deformity. Her nasal denuded the epithelium of the alar base flap (D-flap)
tip was augmented with a conchal cartilage graft and and pulled it under the lateral tip of flap C. In the present
her nostril sill was reduced with a medially based de- study, we used a medially based de-epithelialized flap
epithelialized flap [Figure 4]. that did not require a pull-out suture or cinching suture in
the nasal septum.
DISCUSSION
In an embryological study, Green found that two
[12]
A nasal base reduction typically involves the soft tissue relevant muscular systems exist: sphincteric fibers
resection of one or more of the nasal bases (ala, sill, below the mucosal surface that are more prominent at
or columellar base). Anatomically, the labio-nostril the nasal sill, and a more superficial layer corresponding
[6]
to the muscles of facial expression. He noted that the
floor angle is approximately 105° and acute. In cleft lip
patients, the labio-nostril floor angle is obtuse due to the lateral external muscle fibers pass around the lower free
border of the alar cartilage to insert into the sphincteric
soft tissue defect of the nostril sill and the supporting muscle.
bony framework. [7]
Recently, Oh et al. observed that the nasalis muscle
[13]
Buried flaps have been used in the lip. [8-11] In order to lies most superficially in the nostril sill, followed by the
shorten the lip, Kostianovsky augmented the upper depressor septi nasi and the orbicularis oris underneath.
[8]
and lower lip using buried de-epithelialized local flaps. In our observations, we did not find the nasalis muscle
In order to improve the senile lip, Guerrissi [9,10] de- in the middle of the nostril sill. Instead, obliquely running
epithelialized a strip of skin on the vermilion border and depressor septi nasi muscle fibers comprised the nostril
buried the remaining dermal flap in the pocket, which sill [Figure 3]. In this study, we observed a depressor
was performed by undermining the skin of the superior septi nasi muscle that ran obliquely and comprised the
third of the upper lip. nostril sill just beneath a thick layer of dermis.
In the above studies, the buried flaps were used to The measurements we used in this patient cohort (alar
augment the upper or lower vermilion. In our study we distance, nostril floor width) supported the proposal that
used a de-epithelialized flap for simultaneous nasal narrowing the alar base is beneficial. The RR of the
base narrowing and nostril sill augmentation. nostril floor was 7.72% ± 3.62%. The RRs of the alar
294 Plastic and Aesthetic Research ¦ Volume 3 ¦ September 20, 2016