
Page 12 - Read Online
P. 12
Liang et al. Plast Aesthet Res 2019;6:23 I http://dx.doi.org/10.20517/2347-9264.2019.33 Page 7 of 9
Positive TDC measurements Positive Risk factors (family
Suspected patients BIS history, acquired
Genetic screening lymphatic damage
etc.)
History Physical examinations Further assessment
symptoms Skin evaluation Positive 3D photography/perometry
Tape measurement/water plethysmography MRI/CT/Ultrasound
Negative
Lymphoscintigraphy Positive
MRL Treatment
ICG lymphography/FML
Negative
Consider other
potential causes
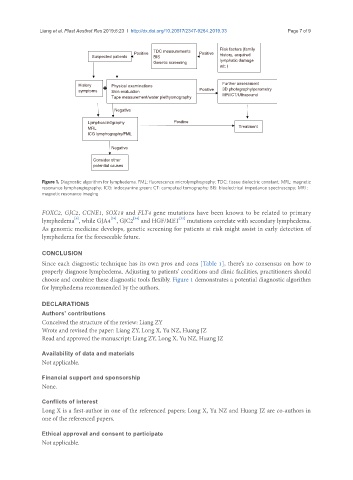
Figure 1. Diagnostic algorithm for lymphedema. FML: fluorescence microlymphography; TDC: tissue dielectric constant; MRL: magnetic
resonance lymphangiography; ICG: indocyanine green; CT: computed tomography; BIS: bioelectrical impedance spectroscopy; MRI:
magnetic resonance imaging
FOXC2, GJC2, CCNE1, SOX18 and FLT4 gene mutations have been known to be related to primary
[9]
[35]
[34]
[34]
lymphedema , while GJA4 , GJC2 and HGF/MET mutations correlate with secondary lymphedema.
As genomic medicine develops, genetic screening for patients at risk might assist in early detection of
lymphedema for the foreseeable future.
CONCLUSION
Since each diagnostic technique has its own pros and cons [Table 1], there’s no consensus on how to
properly diagnose lymphedema. Adjusting to patients’ conditions and clinic facilities, practitioners should
choose and combine these diagnostic tools flexibly. Figure 1 demonstrates a potential diagnostic algorithm
for lymphedema recommended by the authors.
DECLARATIONS
Authors’ contributions
Conceived the structure of the review: Liang ZY
Wrote and revised the paper: Liang ZY, Long X, Yu NZ, Huang JZ
Read and approved the manuscript: Liang ZY, Long X, Yu NZ, Huang JZ
Availability of data and materials
Not applicable.
Financial support and sponsorship
None.
Conflicts of interest
Long X is a first-author in one of the referenced papers; Long X, Yu NZ and Huang JZ are co-authors in
one of the referenced papers.
Ethical approval and consent to participate
Not applicable.