
Page 35 - Read Online
P. 35
Ciria et al. Mini-invasive Surg 2024;8:10 https://dx.doi.org/10.20517/2574-1225.2023.126 Page 3 of 9
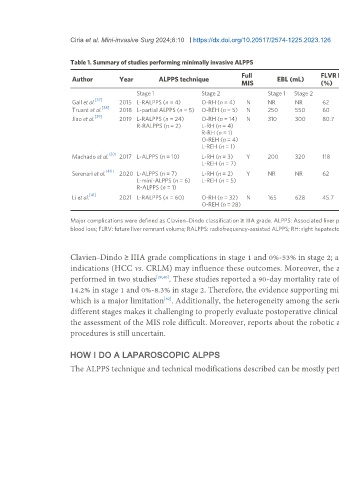
Table 1. Summary of studies performing minimally invasive ALPPS
Full FLVR hypertrophy Length of hospital stay Major complications 90-day mortality
Author Year ALPPS technique EBL (mL)
MIS (%) (days) (%) (%)
Stage 1 Stage 2 Stage 1 Stage 2 Stage 1 Stage 2 Stage 1 Stage 2
[37]
Gall et al. 2015 L-RALPPS (n = 4) O-RH (n = 4) N NR NR 62 NR NR 20 NR 0
[38]
Truant et al. 2018 L-partial ALPPS (n = 5) O-REH (n = 5) N 250 550 60 7 12 0 40 0
[39]
Jiao et al. 2019 L-RALPPS (n = 24) O-RH (n = 14) N 310 300 80.7 9.5 8 3.85 15.3 3.8
R-RALPPS (n = 2) L-RH (n = 4)
R-RH (n = 1)
O-REH (n = 4)
L-REH (n = 1)
[20]
Machado et al. 2017 L-ALPPS (n = 10) L-RH (n = 3) Y 200 320 118 NR NR 0 0 0
L-REH (n = 7)
[40]
Serenari et al. 2020 L-ALPPS (n = 7) L-RH (n = 2) Y NR NR 62 6.5 12 14.2 8.3 0
L-mini-ALPPS (n = 6) L-REH (n = 5)
R-ALPPS (n = 1)
[41]
Li et al. 2021 L-RALPPS (n = 60) O-RH (n = 32) N 165 628 45.7 NR 23.4 13.3 53.3 0
O-REH (n = 28)
Major complications were defined as Clavien–Dindo classification ≥ IIIA grade. ALPPS: Associated liver partition with portal vein ligation for staged hepatectomy; MIS: minimally invasive surgery; EBL: estimated
blood loss; FLRV: future liver remnant volume; RALPPS: radiofrequency-assisted ALPPS; RH: right hepatectomy; REH: right extended hepatectomy; NR: Not Reported; N: not; Y: yes.
Clavien–Dindo ≥ IIIA grade complications in stage 1 and 0%-53% in stage 2; and (b) the highest 90-day mortality rate reported was 3.8%. Case selection and
indications (HCC vs. CRLM) may influence these outcomes. Moreover, the approach performed during stages is biased. Only the full MIS procedure was
performed in two studies [20,40] . These studies reported a 90-day mortality rate of 0% and a Clavien–Dindo ≥ IIIA grade complication rate of approximately 0%-
14.2% in stage 1 and 0%-8.3% in stage 2. Therefore, the evidence supporting minimal invasiveness is weak and mainly supported by case reports or case series,
which is a major limitation . Additionally, the heterogeneity among the series concerning the ALPPS techniques performed, indications or approaches in
[42]
different stages makes it challenging to properly evaluate postoperative clinical outcomes. Evidence about open versus modified MI-ALPPS is lacking, making
the assessment of the MIS role difficult. Moreover, reports about the robotic approach are limited. Considering these issues, the influence of MIS in ALPPS
procedures is still uncertain.
HOW I DO A LAPAROSCOPIC ALPPS
The ALPPS technique and technical modifications described can be mostly performed by a minimally invasive approach, always in experienced hands. A step-