
Page 78 - Read Online
P. 78
Page 4 of 8 Ban et al. Hepatoma Res 2021;7:13 I http://dx.doi.org/10.20517/2394-5079.2020.104
C
A
B
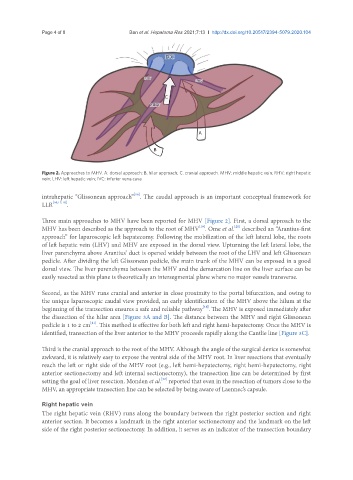
Figure 2. Approaches to MHV. A: dorsal approach; B. hilar approach; C. cranial approach. MHV: middle hepatic vein; RHV: right hepatic
vein; LHV: left hepatic vein; IVC: inferior vena cava
[16]
intrahepatic “Glissonean approach” . The caudal approach is an important conceptual framework for
LLR [10,17,18] .
Three main approaches to MHV have been reported for MHV [Figure 2]. First, a dorsal approach to the
MHV has been described as the approach to the root of MHV . Ome et al. described an “Arantius-first
[20]
[19]
approach” for laparoscopic left hepatecomy. Following the mobilization of the left lateral lobe, the roots
of left hepatic vein (LHV) and MHV are exposed in the dorsal view. Upturning the left lateral lobe, the
liver parenchyma above Arantius’ duct is opened widely between the root of the LHV and left Glissonean
pedicle. After dividing the left Glissonean pedicle, the main trunk of the MHV can be exposed in a good
dorsal view. The liver parenchyma between the MHV and the demarcation line on the liver surface can be
easily resected as this plane is theoretically an intersegmental plane where no major vessels transverse.
Second, as the MHV runs cranial and anterior in close proximity to the portal bifurcation, and owing to
the unique laparoscopic caudal view provided, an early identification of the MHV above the hilum at the
beginning of the transection ensures a safe and reliable pathway . The MHV is exposed immediately after
[18]
the dissection of the hilar area [Figure 3A and B]. The distance between the MHV and right Glissonean
[21]
pedicle is 1 to 2 cm . This method is effective for both left and right hemi-hepatectomy. Once the MHV is
identified, transection of the liver anterior to the MHV proceeds rapidly along the Cantlie line [Figure 3C].
Third is the cranial approach to the root of the MHV. Although the angle of the surgical device is somewhat
awkward, it is relatively easy to expose the ventral side of the MHV root. In liver resections that eventually
reach the left or right side of the MHV root (e.g., left hemi-hepatectomy, right hemi-hepatectomy, right
anterior sectionectomy and left internal sectionectomy), the transection line can be determined by first
[22]
setting the goal of liver resection. Monden et al. reported that even in the resection of tumors close to the
MHV, an appropriate transection line can be selected by being aware of Laennec’s capsule.
Right hepatic vein
The right hepatic vein (RHV) runs along the boundary between the right posterior section and right
anterior section. It becomes a landmark in the right anterior sectionectomy and the landmark on the left
side of the right posterior sectionectomy. In addition, it serves as an indicator of the transection boundary