
Page 103 - Read Online
P. 103
Page 12 of 18 Thiruchelvam et al. Hepatoma Res 2021;7:22 I http://dx.doi.org/10.20517/2394-5079.2020.144
A B
C D
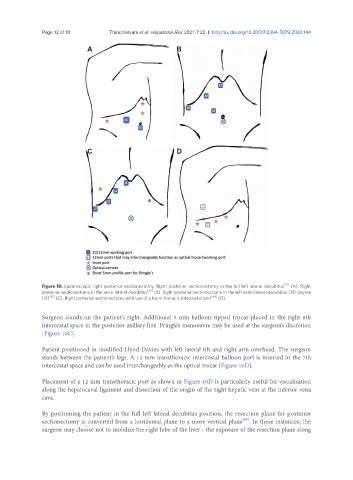
Figure 10. Laparoscopic right posterior sectionectomy. Right posterior sectionectomy in the full left lateral decubitus [41] (A). Right
posterior sectionectomy in the semi-lateral decubitus [42] (B). Right posterior sectionectomy in the left semi-lateral decubitus (30-degree
tilt) [43] (C). Right posterior sectionectomy with use of a trans-thoracic intercostal port [44] (D).
Surgeon stands on the patient’s right. Additional 5 mm balloon-tipped trocar placed in the right 8th
intercostal space in the posterior axillary line. Pringle’s manoeuvre may be used at the surgeon’s discretion
[Figure 10C].
Patient positioned in modified Llyod-Davies with left lateral tilt and right arm overhead. The surgeon
stands between the patient’s legs. A 12 mm transthoracic intercostal balloon port is inserted in the 7th
intercostal space and can be used interchangeably as the optical trocar [Figure 10D].
Placement of a 12 mm transthoracic port as shown in Figure 10D is particularly useful for visualisation
along the hepatocaval ligament and dissection of the origin of the right hepatic vein at the inferior vena
cava.
By positioning the patient in the full left lateral decubitus position, the resection plane for posterior
[45]
sectionectomy is converted from a horizontal plane to a more vertical plane . In these instances, the
surgeon may choose not to mobilize the right lobe of the liver - the exposure of the resection plane along