
Page 310 - Read Online
P. 310
Page 8 of 19 Cervantes-Gracia et al. Vessel Plus 2020;4:27 I http://dx.doi.org/10.20517/2574-1209.2020.22
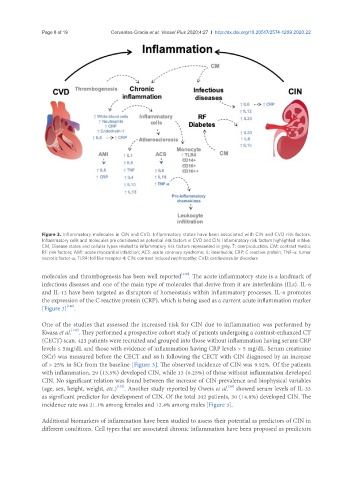
Figure 3. Inflammatory molecules in CIN and CVD. Inflammatory states have been associated with CIN and CVD risk factors.
Inflammatory cells and molecules are considered as potential risk factors in CVD and CIN. Inflammatory risk factors highlighted in blue.
CM, Disease states and cellular types related to inflammatory risk factors represented in grey. ↑: overproduction. CM: contrast media;
RF: risk factors; AMI: acute myocardial infarction; ACS: acute coronary syndrome; IL: interleukin; CRP: C reactive protein; TNF-a: tumor
necrotic factor-a; TLR4: toll like receptor 4; CIN: contrast induced nephropathy; CVD: cardiovascular disorders
[139]
molecules and thrombogenesis has been well reported . The acute inflammatory state is a landmark of
infectious diseases and one of the main type of molecules that derive from it are interleukins (ILs). IL-6
and IL-12 have been targeted as disruptors of homeostasis within inflammatory processes. IL-6 promotes
the expression of the C reactive protein (CRP), which is being used as a current acute inflammation marker
[140]
[Figure 3] .
One of the studies that assessed the increased risk for CIN due to inflammation was performed by
[132]
Kwasa et al. . They performed a prospective cohort study of patients undergoing a contrast-enhanced CT
(CECT) scan. 423 patients were recruited and grouped into those without inflammation having serum CRP
levels ≤ 5mg/dL and those with evidence of inflammation having CRP levels > 5 mg/dL. Serum creatinine
(SCr) was measured before the CECT and 48 h following the CECT with CIN diagnosed by an increase
of > 25% in SCr from the baseline [Figure 3]. The observed incidence of CIN was 9.92%. Of the patients
with inflammation, 29 (13.5%) developed CIN, while 13 (6.25%) of those without inflammation developed
CIN. No significant relation was found between the increase of CIN prevalence and biophysical variables
[30]
(age, sex, height, weight, etc.) . Another study reported by Oweis et al. showed serum levels of IL-33
[132]
as significant predictor for development of CIN. Of the total 202 patients, 30 (14.8%) developed CIN. The
incidence rate was 21.1% among females and 12.4% among males [Figure 3].
Additional biomarkers of inflammation have been studied to assess their potential as predictors of CIN in
different conditions. Cell types that are associated chronic inflammation have been proposed as predictors