
Page 183 - Read Online
P. 183
Page 4 of 7 Patel et al. Plast Aesthet Res 2020;7:18 I http://dx.doi.org/10.20517/2347-9264.2019.15
Table 1. Regional flap options for abdominal wall soft tissue reconstruction
Flap name Donor site Possible recipient sites Pedicle Components Disadvantages
ALT [11] Anterolateral Infraumbilical abdomen Descending branch of the Fasciocutaneous Limited arc of rotation
thigh lateral femoral circumflex Flap width limited to 8 cm to permit
primary closure of thigh donor site
External oblique [7] Anterolateral Upper two thirds of the Lateral branches of Myocutaneous Limited arc of rotation
abdominal wall abdominal wall posterior intercostal vessels Distal flap tip perfusion unreliable in
fasciocutaneous design
TFL [8,9] Lateral thigh Lower two thirds of the Ascending branch of lateral Myocutaneous Unreliability of distal one third of
abdominal wall femoral circumflex artery skin paddle
Rectus femoris [10] Anterior thigh Lower two thirds of the Descending branch of Myocutaneous Donor site morbidity and limited
abdominal wall lateral femoral circumflex terminal knee extension
artery
Omentum [12] Omentum Entire abdominal wall Right or left gastroepiploic Fat, connective Omentum must be resurfaced with
arteries tissue and a skin graft
lymphatics Potential for intraabdominal injury
Subtotal thigh [13] Thigh Entire abdominal wall Lateral circumflex femoral Fasciocutaneous Skin grafted donor site
artery or myocutaneous Limited terminal knee extension
with inclusion of rectus femoris
ALT: anterolateral thighfasciocutaneous; TFL: tensor fascia lata myocutaneous
A B C
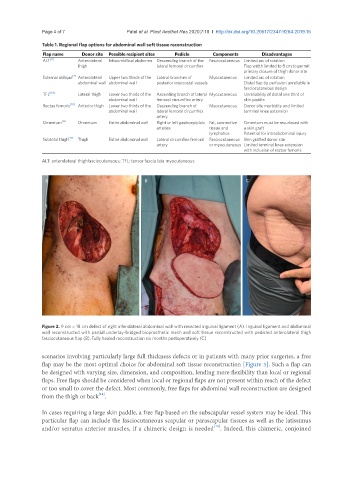
Figure 2. 9 cm × 18 cm defect of right inferolateral abdominal wall with resected inguinal ligament (A). Inguinal ligament and abdominal
wall reconstructed with partial underlay-bridged bioprosthetic mesh and soft tissue reconstructed with pedicled anterolateral thigh
fasciocutaneous flap (B). Fully healed reconstruction six months postoperatively (C)
scenarios involving particularly large full thickness defects or in patients with many prior surgeries, a free
flap may be the most optimal choice for abdominal soft tissue reconstruction [Figure 3]. Such a flap can
be designed with varying size, dimension, and composition, lending more flexibility than local or regional
flaps. Free flaps should be considered when local or regional flaps are not present within reach of the defect
or too small to cover the defect. Most commonly, free flaps for abdominal wall reconstruction are designed
[14]
from the thigh or back .
In cases requiring a large skin paddle, a free flap based on the subscapular vessel system may be ideal. This
particular flap can include the fasciocutaneous scapular or parascapular tissues as well as the latissimus
and/or serratus anterior muscles, if a chimeric design is needed . Indeed, this chimeric, conjoined
[15]