
Page 230 - Read Online
P. 230
Page 6 of 20 Siegal et al. Plast Aesthet Res 2019;6:25 I http://dx.doi.org/10.20517/2347-9264.2019.35
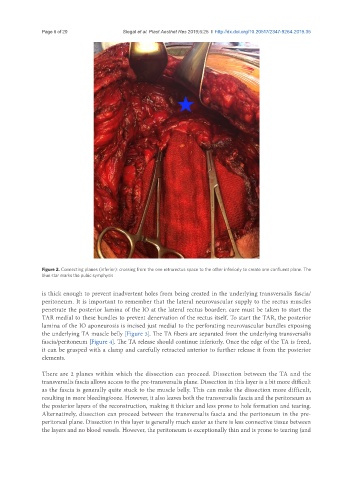
Figure 2. Connecting planes (inferior): crossing from the one retrorectus space to the other inferiorly to create one confluent plane. The
blue star marks the pubic symphysis
is thick enough to prevent inadvertent holes from being created in the underlying transversalis fascia/
peritoneum. It is important to remember that the lateral neurovascular supply to the rectus muscles
penetrate the posterior lamina of the IO at the lateral rectus boarder; care must be taken to start the
TAR medial to these bundles to prevent denervation of the rectus itself. To start the TAR, the posterior
lamina of the IO aponeurosis is incised just medial to the perforating neurovascular bundles exposing
the underlying TA muscle belly [Figure 3]. The TA fibers are separated from the underlying transversalis
fascia/peritoneum [Figure 4]. The TA release should continue inferiorly. Once the edge of the TA is freed,
it can be grasped with a clamp and carefully retracted anterior to further release it from the posterior
elements.
There are 2 planes within which the dissection can proceed. Dissection between the TA and the
transversalis fascia allows access to the pre-transversalis plane. Dissection in this layer is a bit more difficult
as the fascia is generally quite stuck to the muscle belly. This can make the dissection more difficult,
resulting in more bleeding/ooze. However, it also leaves both the transversalis fascia and the peritoneum as
the posterior layers of the reconstruction, making it thicker and less prone to hole formation and tearing.
Alternatively, dissection can proceed between the transversalis fascia and the peritoneum in the pre-
peritoneal plane. Dissection in this layer is generally much easier as there is less connective tissue between
the layers and no blood vessels. However, the peritoneum is exceptionally thin and is prone to tearing (and