
Page 154 - Read Online
P. 154
Fariña et al. Skeletal anchorage for rigid external distractor
This study aimed to overcome some of these
limitations by modifying the method by which facial
bones are anchored to an extraoral distraction device,
specifically RED II. Several authors [1,5,10,11] describe
one of the limitations being the need for teeth to be
used as anchorage. Regardless of the dentition phase,
they need to be in good and healthy condition. In
the proposed technique, the pyriform apertures and
infraorbital rims are used as anchorage points and teeth
are only necessary to stabilize the distracted segments
once they have achieved the desired occlusion.
Figure 3: Cone beam computed tomography showing the wires Nevertheless, as Nishimoto et al. [18] emphasised,
anchored directly to the bone the presence of teeth is ideal because it diminishes
the chance of relapse, since occlusion holds skeletal
DISCUSSION bases in position. Furthermore, they state that when
teeth are missing, consolidation time should be longer.
Distraction osteogenesis was introduced in the
craniofacial field in 1992 by McCarthy et al. [13] to correct In the publication by Nout et al. [10] an alternative is
mandibular hypoplasia. [14] The procedure has since mentioned for distraction with RED without dental
anchoring in a patient diagnosed with Pfeiffer’s
been widely used in the field of craniofacial surgery,
and is considered today as an alternative method to syndrome. They suggested using bilateral anchorage
to the pyriform aperture only, fixed with screws. SARED
treating craniofacial dysplasia. [5,15] Intra and extraoral does not require the use of osteosynthesis (plates nor
distraction devices can be used. Extraoral devices are screws) nor a custom-made intraoral orthodontic splint,
easier to handle, allow for more force to be applied and reducing the cost of treatment and diminishing the risk
for greater advancement to be achieved. They also of damage of dental follicles and roots.
allow modification and better control of the distraction
vector. [6,15,16] When an extraoral device is used, further Since teeth anchoring is unnecessary in SARED, the
surgery is not needed to remove the distractor. [6,17] force can be applied directly to the bone. This in turn
A C E G
B D F H
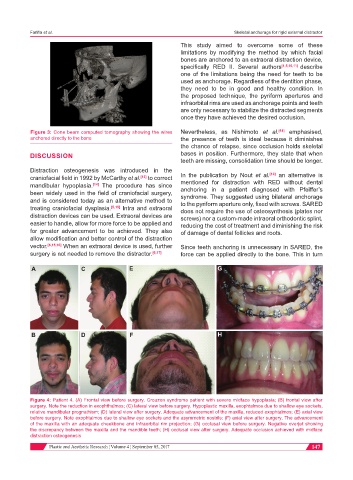
Figure 4: Patient 4. (A) Frontal view before surgery. Crouzon syndrome patient with severe midface hypoplasia; (B) frontal view after
surgery. Note the reduction in exophthalmos; (C) lateral view before surgery. Hypoplastic maxilla, exophtalmos due to shallow eye sockets,
relative mandibular prognathism; (D) lateral view after surgery. Adequate advancement of the maxilla, reduced exophtalmos; (E) axial view
before surgery. Note exophtalmos due to shallow eye sockets and the asymmetric nostrils; (F) axial view after surgery. The advancement
of the maxilla with an adequate cheekbone and infraorbital rim projection; (G) occlusal view before surgery. Negative overjet showing
the discrepancy between the maxilla and the mandible teeth; (H) occlusal view after surgery. Adequate occlusion achieved with midface
distraction osteogenesis
Plastic and Aesthetic Research ¦ Volume 4 ¦ September 05, 2017 147