
Page 93 - Read Online
P. 93
inframammary crease distance, was 11 cm bilaterally with general anesthesia with the patient in supine position
a bilateral sliding ptosis of the skin envelope. and arms abducted < 90°. Patient received a single
dose of Cephalosporin intraoperatively. Cross‑hatched
Preoperative discussion primarily centered on the size
of her breast and breast esthetics following explantation area and medially based flap was de‑epithelialized
alone. She was informed that her breasts were likely to leaving 4.5 cm Neo NAC. Intervening tissue between
look very saggy if explantation alone was performed and the markings and de‑epithelialized area was excised
if a simultaneous mastopexy was carried out, especially (right 87 gm and left 119 gm) [Figure 3]. Both implants
using a Wise Pattern markings, resultant tissue excision were removed, and both showed malorientation, fold
would reduce her breast to a small B cup at the most. flaw failures with a rupture on the right side [Figure 4].
Autologous breast remodeling was discussed either De‑epithelialized inferior dermoglandular flap was pulled
using fat transfer as a secondary procedure or using up and stitched to pectoralis major, without tension
de‑epithelialized inferior dermoglandular flap as volume and using 2‑0 vicryl sutures [Figure 5]. Hemostasis was
conservation and remodeling in the same setting. She performed, and skin closure done using 3‑0 vicryl and
showed her interest in the later procedure. The procedure 4‑0 monocryl and 4‑0 monocryl was used suture to NAC.
was planned under general anesthetic and as a day case. No drains were used, and patient was discharged on the
same day. The patient was followed one and 3 weeks
Markings and technique postoperatively, she had no neck or backache, her bra cup
Patient was marked in standing position. Neo nipple areolar size was measured 34 C and was extremely pleased with
complex (NAC) was marked at 21 cm using infra‑mammary the results [Figures 6‑8].
crease as a reference [Figure 1]. Wise pattern markings
were used for skin reduction with a medially based flap. DISCUSSION
A transversely oriented skin area, to be de‑zepithelialized,
was marked and cross‑hatched below 7 cm vertical limbs Augmentation mammoplasty is one of the most
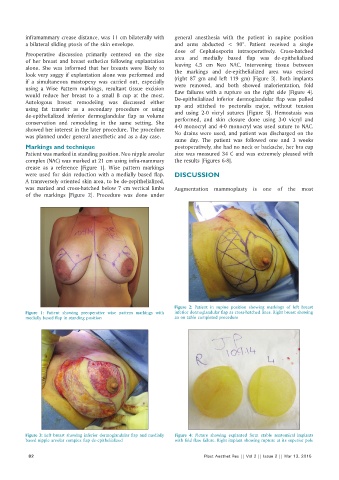
of the markings [Figure 2]. Procedure was done under
Figure 2: Patient in supine position showing markings of left breast
Figure 1: Patient showing preoperative wise pattern markings with inferior dermoglandular flap as cross‑hatched lines. Right breast showing
medially based flap in standing position an on table completed procedure
Figure 3: Left breast showing inferior dermoglandular flap and medially Figure 4: Picture showing explanted form stable anatomical implants
based nipple areolar complex flap de‑epithelialized with fold flaw failure. Right implant showing rupture at its superior pole
82 Plast Aesthet Res || Vol 2 || Issue 2 || Mar 13, 2015