
Page 155 - Read Online
P. 155
Later, the patient presented with a residual mass over left It was decided to cover the defect with TFL pedicle flap.
inguinal region. There was a hard swelling of 4 cm × 3 cm We followed the same technique of harvesting of TFL as
with restricted mobility in left inguinal region [Figure 1]. described by various authors. [2,4] The donor flap outlining
Also, multiple small lymph nodes were palpable on the was done with U-shaped incision on the thigh. The elevation
right side, the largest measuring 1 cm × 1 cm. was carried out in a subfascial plane from distal to proximal.
The lateral circumflex femoral artery was then easily
Magnetic resonance image of the left inguinal region
showed enlarged necrotic lymph node, anterior to femoral identified high up as it passes between the rectus femoris
vessels in the subcutaneous plane. There was a loss of fat and the vastus lateralis, where it gives the transverse
planes with left femoral vein. Left femoral artery and right branch, which pierces the TFL muscle accompanied by venae
inguinal region were normal. Fine needle aspiration cytology comitantes. Then dissection was performed to sufficiently
was done from bilateral inguinal lymph nodes. The left mobilize the flap for proper defect coverage [Figure 3]. The
inguinal lymph node showed squamous cell carcinomatous medial end of the incision was joined to the lateral aspect
deposit. The right inguinal lymph nodes were reactive of the inguinal defect. The free end of the flap was then
in nature without any tumor deposit. Chest X-ray was rotated upward and medially [Figure 4] and sutured to the
reported as normal. Routine hematological and biochemical defect created by the inguinal dissection. Donor site could
investigations like complete hemogram, serum urea and be approximated without any tension [Figure 5]. Drain was
creatine were within normal limit. Viral markers like human placed, and wound was closed in layers.
retroviral antigen, hepatitis B and C were also negative. Postoperative period was uneventful. Flap was healthy
He underwent left ilioinguinal block dissection. on the seventh postoperative day, and the patient was
Perioperatively, there were necrotic lymph nodes of discharged. He was advised to undergo regular follow-up.
4 cm × 4 cm in size, abutting the femoral vein. Multiple Suture and skin stapler was removed on the 14th day.
lymph nodes were present in iliac region, largest There was no necrosis or dehiscence, and the cosmesis
measuring 3 cm × 1 cm. The Cloquet lymph node was was acceptable.
also present. Three cm skin margin was taken beyond the Other options for alternative flaps in this case would
indurated area thereby creating a defect of 8 cm × 8 cm have been perforator based anterolateral thigh (ALT)
in the left inguinal region [Figure 2].
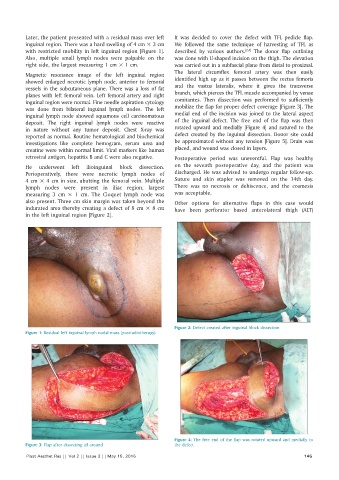
Figure 2: Defect created after inguinal block dissection
Figure 1: Residual left inguinal lymph nodal mass (postradiotherapy)
Figure 4: The free end of the flap was rotated upward and medially to
Figure 3: Flap after dissecting all around the defect
Plast Aesthet Res || Vol 2 || Issue 3 || May 15, 2015 145