
Page 99 - Read Online
P. 99
Vakhshori et al. Plast Aesthet Res 2023;10:36 https://dx.doi.org/10.20517/2347-9264.2022.78 Page 13 of 22
brachial artery, or
thoracoacromial
vessels
[66]
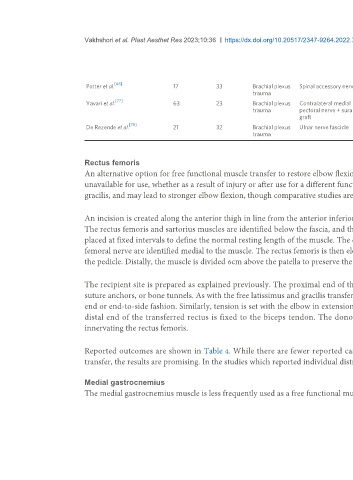
Potter et al. 17 33 Brachial plexus Spinal accessory nerve Thoracoacromial 2 0 15 92 1 exploration for
trauma artery; cephalic vein venous congestion
[77]
Yavari et al. 63 23 Brachial plexus Contralateral medial Brachial artery 16 26 21 NR 2 flap failures
trauma pectoral nerve + sural
graft
[78]
De Rezende et al. 21 32 Brachial plexus Ulnar nerve fascicle Thoracoacromial 3 5 13 86 None reported
trauma artery and vein
Rectus femoris
An alternative option for free functional muscle transfer to restore elbow flexion is the use of rectus femoris. This may be useful when the gracilis muscles are
unavailable for use, whether as a result of injury or after use for a different function. The rectus femoris is a fusiform muscle that generates more force than the
gracilis, and may lead to stronger elbow flexion, though comparative studies are lacking .
[79]
An incision is created along the anterior thigh in line from the anterior inferior iliac spine to the patella. A skin paddle may be incorporated into the incision.
The rectus femoris and sartorius muscles are identified below the fascia, and the sartorius is retracted medially. As mentioned above, marking sutures may be
placed at fixed intervals to define the normal resting length of the muscle. The descending branch of the lateral femoral circumflex vessels and branches of the
femoral nerve are identified medial to the muscle. The rectus femoris is then elevated from distal to proximal and lateral to medial with care to avoid injury to
the pedicle. Distally, the muscle is divided 6cm above the patella to preserve the quadriceps tendon .
[79]
The recipient site is prepared as explained previously. The proximal end of the muscle is fixed to the coracoid or lateral clavicle and acromion with suture,
suture anchors, or bone tunnels. As with the free latissimus and gracilis transfers, the pedicle anastomosis can be performed to an available artery in an end-to-
end or end-to-side fashion. Similarly, tension is set with the elbow in extension to restore the distance between the previously placed marking sutures and the
distal end of the transferred rectus is fixed to the biceps tendon. The donor nerve of choice is then sutured to the motor branch of the femoral nerve
innervating the rectus femoris.
Reported outcomes are shown in Table 4. While there are fewer reported cases using a rectus femoris muscle transfer compared to latissimus or gracilis
transfer, the results are promising. In the studies which reported individual distributions of motor grades, 83% achieved at least antigravity strength.
Medial gastrocnemius
The medial gastrocnemius muscle is less frequently used as a free functional muscle transfer option for restoration of elbow flexion, which may be used if other