
Page 102 - Read Online
P. 102
Vakhshori et al. Plast Aesthet Res 2023;10:36 https://dx.doi.org/10.20517/2347-9264.2022.78 Page 15 of 22
Table 5. Reported outcomes of free medial gastrocnemius transfer. MRC: Medical Research Council muscle grade
Elbow Mean
Number Mean
Reference of age Pathology Neurotization Vessel flexion MRC MRC elbow Complications
anastomosis
≥ 4
flexion
MRC < 3
patients (years)
3 (degrees)
De Moraes 7 28 Brachial Ulnar nerve Thoracodorsal 0 3 4 83 None reported
et al. [34] plexus fascicle artery;
trauma Intercostal thoracodorsal
nerve vein and cephalic
Spinal accessory vein
nerve
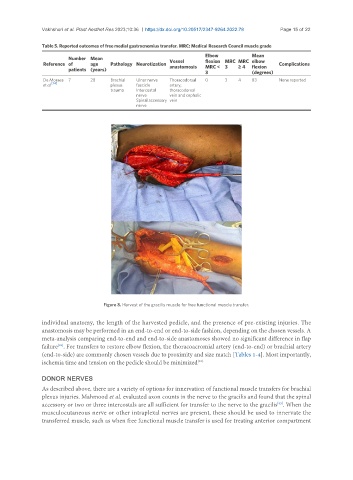
Figure 8. Harvest of the gracilis muscle for free functional muscle transfer.
individual anatomy, the length of the harvested pedicle, and the presence of pre-existing injuries. The
anastomosis may be performed in an end-to-end or end-to-side fashion, depending on the chosen vessels. A
meta-analysis comparing end-to-end and end-to-side anastomoses showed no significant difference in flap
failure . For transfers to restore elbow flexion, the thoracoacromial artery (end-to-end) or brachial artery
[82]
(end-to-side) are commonly chosen vessels due to proximity and size match [Tables 1-4]. Most importantly,
ischemia time and tension on the pedicle should be minimized [48].
DONOR NERVES
As described above, there are a variety of options for innervation of functional muscle transfers for brachial
plexus injuries. Mahmood et al. evaluated axon counts in the nerve to the gracilis and found that the spinal
[83]
accessory or two or three intercostals are all sufficient for transfer to the nerve to the gracilis . When the
musculocutaneous nerve or other intraplexal nerves are present, these should be used to innervate the
transferred muscle, such as when free functional muscle transfer is used for treating anterior compartment