
Page 41 - Read Online
P. 41
Page 6 of 11 Gimenez et al. Plast Aesthet Res 2022;9:28 https://dx.doi.org/10.20517/2347-9264.2021.129
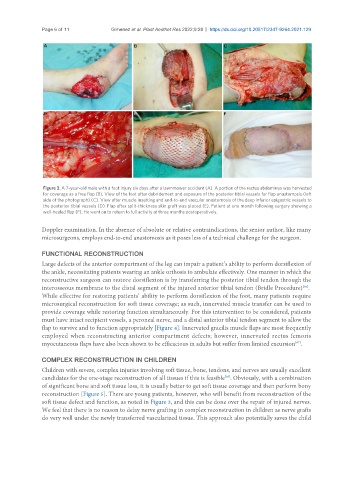
Figure 3. A 7-year-old male with a foot injury six days after a lawnmower accident (A). A portion of the rectus abdominus was harvested
for coverage as a free flap (B). View of the foot after debridement and exposure of the posterior tibial vessels for flap anastomosis (left
side of the photograph) (C). View after muscle insetting and end-to-end vascular anastomosis of the deep inferior epigastric vessels to
the posterior tibial vessels (D). Flap after split-thickness skin graft was placed (E). Patient at one month following surgery showing a
well-healed flap (F). He went on to return to full activity at three months postoperatively.
Doppler examination. In the absence of absolute or relative contraindications, the senior author, like many
microsurgeons, employs end-to-end anastomosis as it poses less of a technical challenge for the surgeon.
FUNCTIONAL RECONSTRUCTION
Large defects of the anterior compartment of the leg can impair a patient’s ability to perform dorsiflexion of
the ankle, necessitating patients wearing an ankle orthosis to ambulate effectively. One manner in which the
reconstructive surgeon can restore dorsiflexion is by transferring the posterior tibial tendon through the
[66]
interosseous membrane to the distal segment of the injured anterior tibial tendon (Bridle Procedure) .
While effective for restoring patients’ ability to perform dorsiflexion of the foot, many patients require
microsurgical reconstruction for soft tissue coverage; as such, innervated muscle transfer can be used to
provide coverage while restoring function simultaneously. For this intervention to be considered, patients
must have intact recipient vessels, a peroneal nerve, and a distal anterior tibial tendon segment to allow the
flap to survive and to function appropriately [Figure 4]. Innervated gracilis muscle flaps are most frequently
employed when reconstructing anterior compartment defects; however, innervated rectus femoris
[67]
myocutaneous flaps have also been shown to be efficacious in adults but suffer from limited excursion .
COMPLEX RECONSTRUCTION IN CHILDREN
Children with severe, complex injuries involving soft tissue, bone, tendons, and nerves are usually excellent
candidates for the one-stage reconstruction of all tissues if this is feasible . Obviously, with a combination
[68]
of significant bone and soft tissue loss, it is usually better to get soft tissue coverage and then perform bony
reconstruction [Figure 5]. There are young patients, however, who will benefit from reconstruction of the
soft tissue defect and function, as noted in Figure 3, and this can be done over the repair of injured nerves.
We feel that there is no reason to delay nerve grafting in complex reconstruction in children as nerve grafts
do very well under the newly transferred vascularized tissue. This approach also potentially saves the child