
Page 131 - Read Online
P. 131
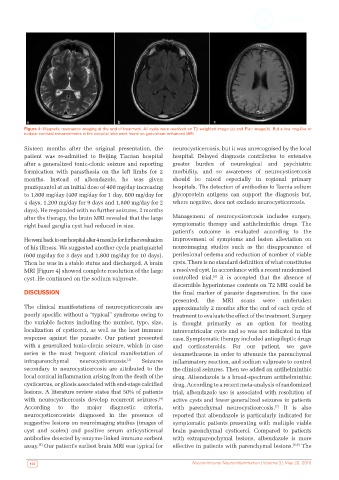
Figure 4: Magnetic resonance imaging at the end of treatment. All cysts were resolved on T2-weighted image (a) and Flair image(b). But a few ring-like or
nodular contrast enhancements in the occipital lobe were found on gadolinium-enhanced MRI
Sixteen months after the original presentation, the neurocysticercosis, but it was unrecognised by the local
patient was re-admitted to Beijing Tiantan hospital hospital. Delayed diagnosis contributes to extensive
after a generalized tonic-clonic seizure and reporting greater burden of neurological and psychiatric
formication with parasthesia on the left limbs for 2 morbidity, and so awareness of neurocysticercosis
months. Instead of albendazole, he was given should be raised especially in regional primary
praziquantel at an initial dose of 400 mg/day increasing hospitals. The detection of antibodies to Taenia solium
to 1,800 mg/day (400 mg/day for 1 day, 600 mg/day for glycoprotein antigens can support the diagnosis but,
4 days, 1,200 mg/day for 9 days and 1,800 mg/day for 2 where negative, does not exclude neurocysticercosis.
days). He responded with no further seizures. 2 months
after the therapy, the brain MRI revealed that the large Management of neurocysticercosis includes surgery,
right basal ganglia cyst had reduced in size. symptomatic therapy and antihelminthic drugs. The
patient’s outcome is evaluated according to the
He went back to our hospital after 4 months for further evaluation improvement of symptoms and lesion alleviation on
of his illness. We suggested another cycle praziquantel neuroimaging studies such as the disappearance of
(600 mg/day for 3 days and 1,800 mg/day for 10 days). perilesional oedema and reduction of number of viable
Then he was in a stable status and discharged. A brain cysts. There is no standard definition of what constitutes
MRI [Figure 4] showed complete resolution of the large a resolved cyst. In accordance with a recent randomised
[6]
cyst. He continued on the sodium valproate. controlled trial, it is accepted that the absence of
discernible hyperintense contents on T2 MRI could be
DISCUSSION the final marker of parasite degeneration. In the case
presented, the MRI scans were undertaken
The clinical manifestations of neurocysticercosis are approximately 2 months after the end of each cycle of
poorly specific without a “typical” syndrome owing to treatment to evaluate the effect of the treatment. Surgery
the variable factors including the number, type, size, is thought primarily as an option for treating
localization of cysticerci, as well as the host immune intraventricular cysts and so was not indicated in this
response against the parasite. Our patient presented case. Symptomatic therapy included antiepileptic drugs
with a generalized tonic-clonic seizure, which in case and corticosteroids. For our patient, we gave
series is the most frequent clinical manifestation of dexamethasone in order to attenuate the parenchymal
intraparenchymal neurocysticercosis. [3] Seizures inflammatory reaction, and sodium valproate to control
secondary to neurocysticercosis are attributed to the the clinical seizures. Then we added an antihelminthic
local cortical inflammation arising from the death of the drug. Albendazole is a broad-spectrum antihelminthic
cysticercus, or gliosis associated with end-stage calcified drug. According to a recent meta-analysis of randomized
lesions. A literature review states that 50% of patients trial, albendazole use is associated with resolution of
with neurocysticercosis develop recurrent seizures. active cysts and fewer generalized seizures in patients
[4]
According to the major diagnostic criteria, with parenchymal neurocysticercosis. It is also
[7]
neurocysticercosisis diagnosed in the presence of reported that albendazole is particularly indicated for
suggestive lesions on neuroimaging studies (images of symptomatic patients presenting with multiple viable
cyst and scolex) and positive serum anticysticercal brain parenchymal cysticerci. Compared to patients
antibodies detected by enzyme-linked immuno sorbent with extraparenchymal lesions, albendazole is more
assay. Our patient’s earliest brain MRI was typical for effective in patients with parenchymal lesions. [8,9] The
[5]
122 Neuroimmunol Neuroinflammation | Volume 3 | May 20, 2016