
Page 173 - Read Online
P. 173
on the OS definitely, although they were not yet fit into
the Cox’s proportional hazards regression model. Given
the small number of patients, these factors cannot
be statistically discarded as a Type II error. Just as in
Glantz’s study, an age > 50, performance status ≤ 70%,
primary tumor (lung cancer, malignant melanoma), and
lack of cytological response present negative prognostic
factors. [29]
Methotrexate is a folate anti-metabolite and a S-phase
specific cytotoxin with a CSF half-life of 4.5-8.0 h. [24]
Therapeutic CSF concentrations obtained in adults and
in children of more than 2 years of age are 12 mg IT MTX
and 1 μmol/L or more during 48-72 h, respectively. [30] IT
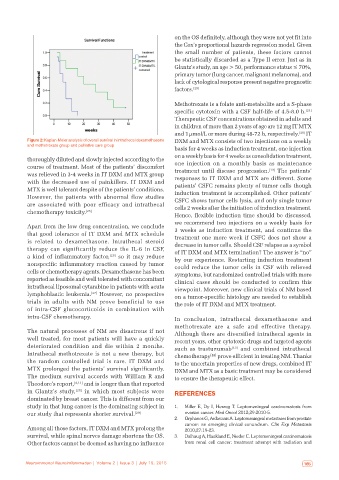
Figure 2: Kaplan‑Meier analysis of overall survival in intrathecal dexamethasone DXM and MTX consists of two injections on a weekly
and methotrexate group and palliative care group
basis for 4 weeks as induction treatment, one injection
on a weekly basis for 4 weeks as consolidation treatment,
thoroughly diluted and slowly injected according to the
course of treatment. Most of the patients’ discomfort one injection on a monthly basis as maintenance
[13]
was relieved in 3-4 weeks in IT DXM and MTX group treatment until disease progression. The patients’
with the decreased use of painkillers. IT DXM and responses to IT DXM and MTX are different. Some
MTX is well tolerant despite of the patients’ conditions. patients’ CSFC remains plenty of tumor cells though
induction treatment is accomplished. Other patients’
However, the patients with abnormal flow studies CSFC shows tumor cells lysis, and only single tumor
are associated with poor efficacy and intrathecal cells 2 weeks after the initiation of induction treatment.
chemotherapy toxicity. [25]
Hence, flexible induction time should be discussed,
we recommend two injections on a weekly basis for
Apart from the low drug concentration, we conclude
that good tolerance of IT DXM and MTX schedule 3 weeks as induction treatment, and continue the
treatment one more week if CSFC does not show a
is related to dexamethasone. Intrathecal steroid decrease in tumor cells. Should CSF relapse as a symbol
therapy can significantly reduce the IL-6 in CSF, of IT DXM and MTX termination? The answer is “no”
a kind of inflammatory factor, [26] so it may reduce by our experience. Restarting induction treatment
nonspecific inflammatory reaction caused by tumor could reduce the tumor cells in CSF with relieved
cells or chemotherapy agents. Dexamethasone has been symptoms, but randomized controlled trials with more
reported as feasible and well tolerated with concomitant clinical cases should be conducted to confirm this
intrathecal liposomal cytarabine in patients with acute viewpoint. Moreover, new clinical trials of NM based
lymphoblastic leukemia. [27] However, no prospective on a tumor-specific histology are needed to establish
trials in adults with NM prove beneficial to use the role of IT DXM and MTX treatment.
of intra-CSF glucocorticoids in combination with
intra-CSF chemotherapy. In conclusion, intrathecal dexamethasone and
methotrexate are a safe and effective therapy.
The natural processes of NM are disastrous if not Although there are diversified intrathecal agents in
well treated, for most patients will have a quickly recent years, other cytotoxic drugs and targeted agents
deteriorated condition and die within 2 months. such as trastuzumab [13] and combined intrathecal
Intrathecal methotrexate is not a new therapy, but chemotherapy prove efficient in treating NM. Thanks
[22]
the random controlled trial is rare. IT DXM and to the uncertain properties of new drugs, combined IT
MTX prolonged the patients’ survival significantly. DXM and MTX as a basic treatment may be considered
The medium survival accords with William R and to ensure the therapeutic effect.
Theodore’s report, [4,11] and is longer than that reported
in Glantz’s study, [28] in which most subjects were REFERENCES
dominated by breast cancer. This is different from our
study in that lung cancer is the dominating subject in 1. Miller E, Dy I, Herzog T. Leptomeningeal carcinomatosis from
our study that represents shorter survival. [29] ovarian cancer. Med Oncol 2012;29:2010‑5.
2. Orphanos G, Ardavanis A. Leptomeningeal metastases from prostate
cancer: an emerging clinical conundrum. Clin Exp Metastasis
Among all those factors, IT DXM and MTX prolong the 2010;27:19‑23.
survival, while spinal nerves damage shortens the OS. 3. Dalhaug A, Haukland E, Nieder C. Leptomeningeal carcinomatosis
Other factors cannot be deemed as having no influence from renal cell cancer: treatment attempt with radiation and
164 Neuroimmunol Neuroinflammation | Volume 2 | Issue 3 | July 15, 2015 Neuroimmunol Neuroinflammation | Volume 2 | Issue 3 | July 15, 2015 165