
Page 207 - Read Online
P. 207
Page 10 of 13 Tang. Mini-invasive Surg 2020;4:24 I http://dx.doi.org/10.20517/2574-1225.2019.60
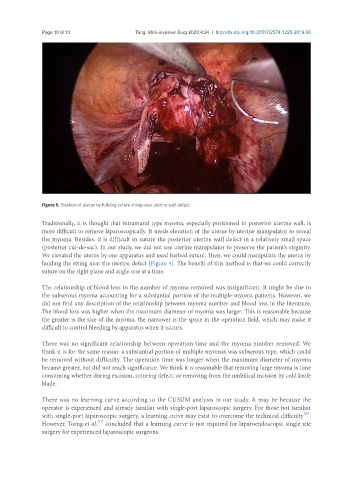
Figure 5. Traction of uterus by holding suture string near uterine wall defect
Traditionally, it is thought that intramural type myoma, especially positioned in posterior uterine wall, is
more difficult to remove laparoscopically. It needs elevation of the uterus by uterine manipulator to reveal
the myoma. Besides, it is difficult in suture the posterior uterine wall defect in a relatively small space
(posterior cul-de-sac). In our study, we did not use uterine manipulator to preserve the patient’s virginity.
We elevated the uterus by one apparatus and used barbed suture. Then, we could manipulate the uterus by
holding the string near the uterine defect [Figure 5]. The benefit of this method is that we could correctly
suture on the right plane and angle one at a time.
The relationship of blood loss to the number of myoma removed was insignificant. It might be due to
the subserous myoma accounting for a substantial portion of the multiple-myoma patients. However, we
did not find any description of the relationship between myoma number and blood loss in the literature.
The blood loss was higher when the maximum diameter of myoma was larger. This is reasonable because
the greater is the size of the myoma, the narrower is the space in the operation field, which may make it
difficult to control bleeding by apparatus when it occurs.
There was no significant relationship between operation time and the myoma number removed. We
think it is for the same reason: a substantial portion of multiple myomas was subserous type, which could
be removed without difficulty. The operation time was longer when the maximum diameter of myoma
became greater, but did not reach significance. We think it is reasonable that removing large myoma is time
consuming whether during excision, suturing defect, or removing from the umbilical incision by cold knife
blade.
There was no learning curve according to the CUSUM analysis in our study. It may be because the
operator is experienced and already familiar with single-port laparoscopic surgery. For those not familiar
[26]
with single-port laparoscopic surgery, a learning curve may exist to overcome the technical difficulty .
[27]
However, Torng et al. concluded that a learning curve is not required for laparoendoscopic single site
surgery for experienced laparoscopic surgeons.