
Page 19 - Read Online
P. 19
Page 6 of 10 Tokairin et al. Mini-invasive Surg 2020;4:32 I http://dx.doi.org/10.20517/2574-1225.2020.23
Figure 7. Dissection of the right recurrent nerve lymph nodes via a right transcervical approach under pneumomediastinum. After the
right common carotid artery is pulled outward and the esophagus is pulled to the left, the right recurrent nerve lymph nodes around the
right subclavian artery are completely retrieved
A B
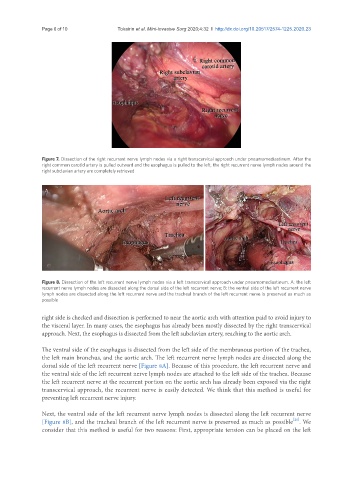
Figure 8. Dissection of the left recurrent nerve lymph nodes via a left transcervical approach under pneumomediastinum. A: the left
recurrent nerve lymph nodes are dissected along the dorsal side of the left recurrent nerve; B: the ventral side of the left recurrent nerve
lymph nodes are dissected along the left recurrent nerve and the tracheal branch of the left recurrent nerve is preserved as much as
possible
right side is checked and dissection is performed to near the aortic arch with attention paid to avoid injury to
the visceral layer. In many cases, the esophagus has already been mostly dissected by the right transcervical
approach. Next, the esophagus is dissected from the left subclavian artery, reaching to the aortic arch.
The ventral side of the esophagus is dissected from the left side of the membranous portion of the trachea,
the left main bronchus, and the aortic arch. The left recurrent nerve lymph nodes are dissected along the
dorsal side of the left recurrent nerve [Figure 8A]. Because of this procedure, the left recurrent nerve and
the ventral side of the left recurrent nerve lymph nodes are attached to the left side of the trachea. Because
the left recurrent nerve at the recurrent portion on the aortic arch has already been exposed via the right
transcervical approach, the recurrent nerve is easily detected. We think that this method is useful for
preventing left recurrent nerve injury.
Next, the ventral side of the left recurrent nerve lymph nodes is dissected along the left recurrent nerve
[21]
[Figure 8B], and the tracheal branch of the left recurrent nerve is preserved as much as possible . We
consider that this method is useful for two reasons: First, appropriate tension can be placed on the left