
Page 34 - Read Online
P. 34
Tschuor et al. Mini-invasive Surg 2020;4:72 I http://dx.doi.org/10.20517/2574-1225.2020.39 Page 3 of 12
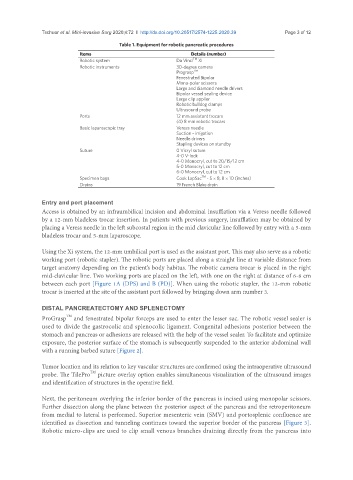
Table 1. Equipment for robotic pancreatic procedures
Items Details (number)
TM
Robotic system Da Vinci Xi
Robotic instruments 30-degree camera
TM
Prograsp
Fenestrated Bipolar
Mono-polar scissors
Large and diamond needle drivers
Bipolar vessel sealing device
Large clip applier
Robotic bulldog clamps
Ultrasound probe
Ports 12 mm assistant trocars
(4) 8 mm robotic trocars
Basic laparoscopic tray Veress needle
Suction - irrigation
Needle drivers
Stapling devices on standby
Suture 0 Vicryl suture
4-0 V-lock
4-0 Monocryl, cut to 20/15/12 cm
5-0 Monocryl, cut to 12 cm
6-0 Monocryl, cut to 12 cm
TM
Specimen bags Cook LapSac - 5 × 8, 8 × 10 (inches)
Drains 19 French Blake drain
Entry and port placement
Access is obtained by an infraumbilical incision and abdominal insufflation via a Veress needle followed
by a 12-mm bladeless trocar insertion. In patients with previous surgery, insufflation may be obtained by
placing a Veress needle in the left subcostal region in the mid clavicular line followed by entry with a 5-mm
bladeless trocar and 5-mm laparoscope.
Using the Xi system, the 12-mm umbilical port is used as the assistant port. This may also serve as a robotic
working port (robotic stapler). The robotic ports are placed along a straight line at variable distance from
target anatomy depending on the patient’s body habitus. The robotic camera trocar is placed in the right
mid-clavicular line. Two working ports are placed on the left, with one on the right at distance of 6-8 cm
between each port [Figure 1A (DPS) and B (PD)]. When using the robotic stapler, the 12-mm robotic
trocar is inserted at the site of the assistant port followed by bringing down arm number 3.
DISTAL PANCREATECTOMY AND SPLENECTOMY
ProGrasp TM and fenestrated bipolar forceps are used to enter the lesser sac. The robotic vessel sealer is
used to divide the gastrocolic and splenocolic ligament. Congenital adhesions posterior between the
stomach and pancreas or adhesions are released with the help of the vessel sealer. To facilitate and optimize
exposure, the posterior surface of the stomach is subsequently suspended to the anterior abdominal wall
with a running barbed suture [Figure 2].
Tumor location and its relation to key vascular structures are confirmed using the intraoperative ultrasound
probe. The TilePro TM picture overlay option enables simultaneous visualization of the ultrasound images
and identification of structures in the operative field.
Next, the peritoneum overlying the inferior border of the pancreas is incised using monopolar scissors.
Further dissection along the plane between the posterior aspect of the pancreas and the retroperitoneum
from medial to lateral is performed. Superior mesenteric vein (SMV) and portosplenic confluence are
identified as dissection and tunneling continues toward the superior border of the pancreas [Figure 3].
Robotic micro-clips are used to clip small venous branches draining directly from the pancreas into