
Page 149 - Read Online
P. 149
Page 8 of 14 Khaitan et al. Mini-invasive Surg 2020;4:51 I http://dx.doi.org/10.20517/2574-1225.2020.34
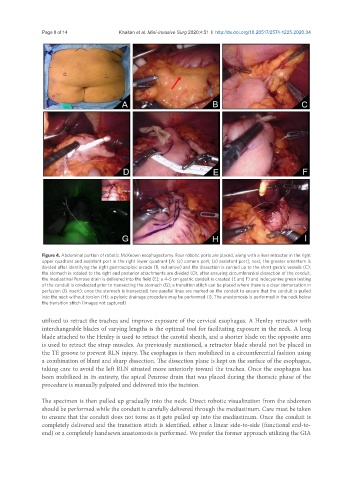
Figure 4. Abdominal portion of robotic McKeown esophagectomy. Four robotic ports are placed, along with a liver retractor in the right
upper quadrant and assistant port in the right lower quadrant [A: (c) camera port; (a) assistant port]; next, the greater omentum is
divided after identifying the right gastroepiploic arcade (B, red arrow) and the dissection is carried up to the short gastric vessels (C);
the stomach is rotated to the right and posterior attachments are divided (D); after ensuring circumferential dissection of the conduit,
the mediastinal Penrose drain is delivered into the field (E); a 4-5 cm gastric conduit is created (E and F) and indocyanine green testing
of the conduit is conducted prior to transecting the stomach (G); a transition stitch can be placed where there is a clear demarcation in
perfusion (G insert); once the stomach is transected, two parallel lines are marked on the conduit to ensure that the conduit is pulled
into the neck without torsion (H); a pyloric drainage procedure may be performed (I). The anastomosis is performed in the neck below
the transition stitch (images not captured)
utilized to retract the trachea and improve exposure of the cervical esophagus. A Henley retractor with
interchangeable blades of varying lengths is the optimal tool for facilitating exposure in the neck. A long
blade attached to the Henley is used to retract the carotid sheath, and a shorter blade on the opposite arm
is used to retract the strap muscles. As previously mentioned, a retractor blade should not be placed in
the TE groove to prevent RLN injury. The esophagus is then mobilized in a circumferential fashion using
a combination of blunt and sharp dissection. The dissection plane is kept on the surface of the esophagus,
taking care to avoid the left RLN situated more anteriorly toward the trachea. Once the esophagus has
been mobilized in its entirety, the apical Penrose drain that was placed during the thoracic phase of the
procedure is manually palpated and delivered into the incision.
The specimen is then pulled up gradually into the neck. Direct robotic visualization from the abdomen
should be performed while the conduit is carefully delivered through the mediastinum. Care must be taken
to ensure that the conduit does not torse as it gets pulled up into the mediastinum. Once the conduit is
completely delivered and the transition stitch is identified, either a linear side-to-side (functional end-to-
end) or a completely handsewn anastomosis is performed. We prefer the former approach utilizing the GIA