
Page 147 - Read Online
P. 147
Page 6 of 14 Khaitan et al. Mini-invasive Surg 2020;4:51 I http://dx.doi.org/10.20517/2574-1225.2020.34
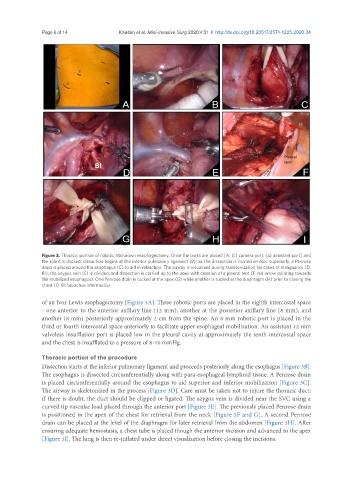
Figure 3. Thoracic portion of robotic McKeown esophagectomy. Once the ports are placed [A: (c) camera port; (a) assistant port] and
the robot is docked, dissection begins at the inferior pulmonary ligament (B); as the dissection is carried en bloc superiorly, a Penrose
drain is placed around the esophagus (C) to aid in retraction. The airway is visualized during skeletonization for cases of malignancy (D;
BI); the azygos vein (E) is divided, and dissection is carried up to the apex with creation of a pleural tent (F, red arrow pointing towards
the mobilized esophagus). One Penrose drain is tucked at the apex (G) while another is tucked at the diaphragm (H) prior to closing the
chest (I). BI: bronchus intermedius
of an Ivor Lewis esophagectomy [Figure 3A]. Three robotic ports are placed in the eighth intercostal space
- one anterior to the anterior axillary line (12 mm), another at the posterior axillary line (8 mm), and
another (8 mm) posteriorly approximately 2 cm from the spine. An 8 mm robotic port is placed in the
third or fourth intercostal space anteriorly to facilitate upper esophageal mobilization. An assistant 12 mm
valveless insufflation port is placed low in the pleural cavity at approximately the tenth intercostal space
and the chest is insufflated to a pressure of 8-10 mmHg.
Thoracic portion of the procedure
Dissection starts at the inferior pulmonary ligament and proceeds posteriorly along the esophagus [Figure 3B].
The esophagus is dissected circumferentially along with para-esophageal lymphoid tissue. A Penrose drain
is placed circumferentially around the esophagus to aid superior and inferior mobilization [Figure 3C].
The airway is skeletonized in the process [Figure 3D]. Care must be taken not to injure the thoracic duct;
if there is doubt, the duct should be clipped or ligated. The azygos vein is divided near the SVC using a
curved tip vascular load placed through the anterior port [Figure 3E]. The previously placed Penrose drain
is positioned in the apex of the chest for retrieval from the neck [Figure 3F and G]. A second Penrose
drain can be placed at the level of the diaphragm for later retrieval from the abdomen [Figure 3H]. After
ensuring adequate hemostasis, a chest tube is placed though the anterior incision and advanced to the apex
[Figure 3I]. The lung is then re-inflated under direct visualization before closing the incisions.