
Page 266 - Read Online
P. 266
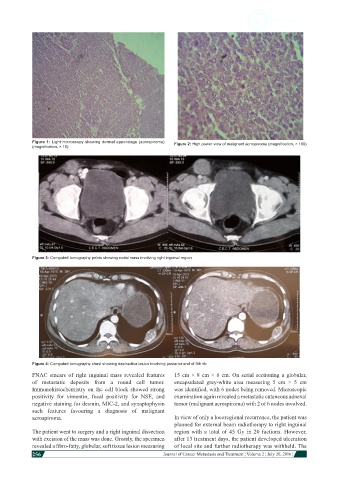
Figure 1: Light microscopy showing dermal appendage (acrospiroma) Figure 2: High power view of malignant acrospiroma (magnification, × 100)
(magnification, × 10)
Figure 3: Computed tomography pelvis showing nodal mass involving right inguinal region
Figure 4: Computed tomography chest showing destructive lesion involving posterior end of 9th rib
FNAC smears of right inguinal mass revealed features 15 cm × 8 cm × 6 cm. On serial sectioning a globular,
of metastatic deposits from a round cell tumor. encapsulated grey-white area measuring 5 cm × 5 cm
Immunohistochemistry on the cell block showed strong was identified, with 6 nodes being removed. Microscopic
positivity for vimentin, focal positivity for NSE, and examination again revealed a metastatic cutaneous adnexal
negative staining for desmin, MIC-2, and synaptophysin tumor (malignant acrospiroma) with 2 of 6 nodes involved.
such features favouring a diagnosis of malignant
acrospiroma. In view of only a locoregional recurrence, the patient was
planned for external beam radiotherapy to right inguinal
The patient went to surgery and a right inguinal dissection region with a total of 45 Gy in 20 factions. However,
with excision of the mass was done. Grossly, the specimen after 13 treatment days, the patient developed ulceration
revealed a fibro-fatty, globular, soft tissue lesion measuring of local site and further radiotherapy was withheld. The
256
Journal of Cancer Metastasis and Treatment ¦ Volume 2 ¦ July 20, 2016 ¦