
Page 31 - Read Online
P. 31
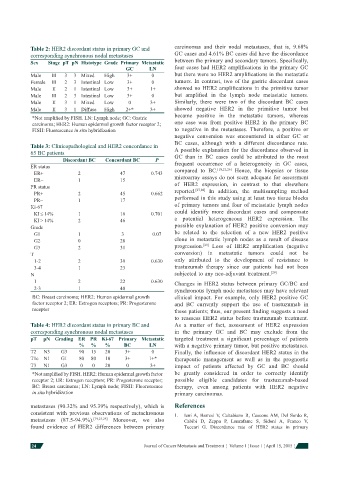
Table 2: HER2 discordant status in primary GC and carcinomas and their nodal metastases, that is, 9.68%
corresponding synchronous nodal metastases GC cases and 4.61% BC cases did have the discordance
Sex Stage pT pN Histotype Grade Primary Metastatic between the primary and secondary tumors. Specifi cally,
GC LN four cases had HER2 amplifi cations in the primary GC
Male III 3 3 Mixed High 3+ 0 but there were no HER2 amplifi cations in the metastatic
Female III 2 3 Intestinal Low 3+ 0 tumors. In contrast, two of the gastric discordant cases
Male II 2 1 Intestinal Low 3+ 1+ showed no HER2 amplifi cations in the primitive tumor
Male III 2 3 Intestinal Low 3+ 0 but amplifi ed in the lymph node metastatic tumors.
Male II 3 1 Mixed Low 0 3+ Similarly, there were two of the discordant BC cases
Male II 3 1 Diffuse High 2+* 3+ showed negative HER2 in the primitive tumor but
became positive in the metastatic tumors, whereas
*Not amplifi ed by FISH. LN: Lymph node; GC: Gastric
carcinoma; HER2: Human epidermal growth factor receptor 2; one case was from positive HER2 in the primary BC
FISH: Fluorescence in situ hybridization to negative in the metastases. Therefore, a positive or
negative conversion was encountered in either GC or
BC cases, although with a different discordance rate.
Table 3: Clinicopathological and HER2 concordance in A possible explanation for the discordance observed in
65 BC patients GC than in BC cases could be attributed to the most
Discordant BC Concordant BC P frequent occurrence of a heterogeneity in GC cases,
ER status compared to BC. [18,21,26] Hence, the biopsies or tissue
ER+ 2 47 0.743 microarray assays do not seem adequate for assessment
ER− 1 15
PR status of HER2 expression, in contrast to that elsewhere
[27,28]
PR+ 2 45 0.662 reported. In addition, the multisampling method
PR− 1 17 performed in this study using at least two tissue blocks
Ki-67 of primary tumors and four of metastatic lymph nodes
KI ≤ 14% 1 16 0.701 could identify more discordant cases and compensate
KI > 14% 2 46 a potential heterogeneous HER2 expression. The
Grade possible explanation of HER2 positive conversion may
G1 1 3 0.07 be related to the selection of a new HER2 positive
G2 0 28 clone in metastatic lymph nodes as a result of disease
G3 2 31 progression. [29] Loss of HER2 amplifi cation (negative
T conversion) in metastatic tumors could not be
1-2 2 39 0.630 only attributed to the development of resistance to
3-4 1 23 trastuzumab therapy since our patients had not been
N subjected to any neo-adjuvant treatment. [29]
1 2 22 0.630 Changes in HER2 status between primary GC/BC and
2-3 1 40 synchronous lymph node metastases may have relevant
BC: Breast carcinoma; HER2: Human epidermal growth clinical impact. For example, only HER2 positive GC
factor receptor 2; ER: Estrogen receptors; PR: Progesterone and BC currently support the use of trastuzumab in
receptor these patients; thus, our present fi nding suggests a need
to reassess HER2 status before trastuzumab treatment.
Table 4: HER2 discordant status in primary BC and As a matter of fact, assessment of HER2 expression
corresponding synchronous nodal metastases in the primary GC and BC may exclude from the
pT pN Grading ER PR Ki-67 Primary Metastatic targeted treatment a signifi cant percentage of patients
% % % BC LN with a negative primary tumor, but positive metastases.
T2 N3 G3 90 15 20 3+ 0 Finally, the infl uence of discordant HER2 status in the
T1c N1 G1 80 80 10 3+ 1+* therapeutic management as well as in the prognostic
T3 N1 G3 0 0 20 0 3+ impact of patients affected by GC and BC should
*Not amplifi ed by FISH. HER2: Human epidermal growth factor be greatly considered in order to correctly identify
receptor 2; ER: Estrogen receptors; PR: Progesterone receptor; possible eligible candidates for trastuzumab-based
BC: Breast carcinoma; LN: Lymph node; FISH: Fluorescence therapy, even among patients with HER2 negative
in situ hybridization primary carcinomas.
metastases (90.32% and 95.39% respectively), which is References
consistent with previous observations of metachronous 1. Ieni A, Barresi V, Caltabiano R, Cascone AM, Del Sordo R,
metastases (87.5-94.9%). [19,23,25] Moreover, we also Cabibi D, Zeppa P, Lanzafame S, Sidoni A, Franco V,
found evidence of HER2 differences between primary Tuccari G. Discordance rate of HER2 status in primary
24 Journal of Cancer Metastasis and Treatment ¦ Volume 1 ¦ Issue 1 ¦ April 15, 2015 ¦