
Page 47 - Read Online
P. 47
Galli et al. J Cancer Metastasis Treat 2022;8:48 https://dx.doi.org/10.20517/2394-4722.2022.19 Page 9 of 14
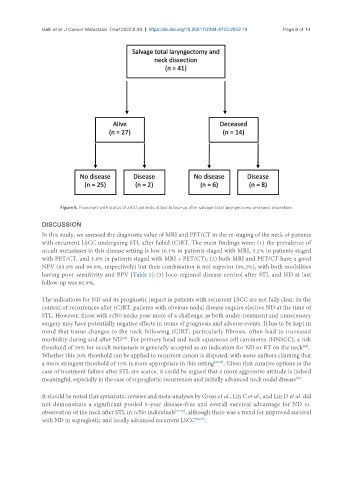
Figure 5. Flowchart with status of all 41 patients at last follow-up after salvage total laryngectomy and neck dissection.
DISCUSSION
In this study, we assessed the diagnostic value of MRI and PET/CT in the re-staging of the neck of patients
with recurrent LSCC undergoing STL after failed (C)RT. The main findings were: (1) the prevalence of
occult metastases in this disease setting is low (6.1% in patients staged with MRI, 3.2% in patients staged
with PET/CT, and 3.8% in patients staged with MRI + PET/CT); (2) both MRI and PET/CT have a good
NPV (93.9% and 96.8%, respectively) but their combination is not superior (96.2%), with both modalities
having poor sensitivity and PPV [Table 3]; (3) loco-regional disease control after STL and ND at last
follow-up was 60.9%.
The indications for ND and its prognostic impact in patients with recurrent LSCC are not fully clear. In the
context of recurrences after (C)RT, patients with obvious nodal disease require elective ND at the time of
STL. However, those with rcN0 necks pose more of a challenge, as both under-treatment and unnecessary
surgery may have potentially negative effects in terms of prognosis and adverse events. It has to be kept in
mind that tissue changes to the neck following (C)RT, particularly fibrosis, often lead to increased
[23]
morbidity during and after ND . For primary head and neck squamous cell carcinoma (HNSCC), a risk
threshold of 20% for occult metastasis is generally accepted as an indication for ND or RT on the neck .
[24]
Whether this 20% threshold can be applied to recurrent cancer is disputed, with some authors claiming that
a more stringent threshold of 15% is more appropriate in this setting [25,26] . Given that curative options in the
case of treatment failure after STL are scarce, it could be argued that a more aggressive attitude is indeed
meaningful, especially in the case of supraglottic recurrences and initially advanced neck nodal disease .
[25]
It should be noted that systematic reviews and meta-analyses by Gross et al., Lin C et al., and Lin D et al. did
not demonstrate a significant pooled 5-year disease-free and overall survival advantage for ND vs.
observation of the neck after STL in rcN0 individuals [27-29] , although there was a trend for improved survival
with ND in supraglottic and locally advanced recurrent LSCC [28,29] .