
Page 647 - Read Online
P. 647
Page 6 of 9 John et al. Hepatoma Res 2020;6:56 I http://dx.doi.org/10.20517/2394-5079.2020.37
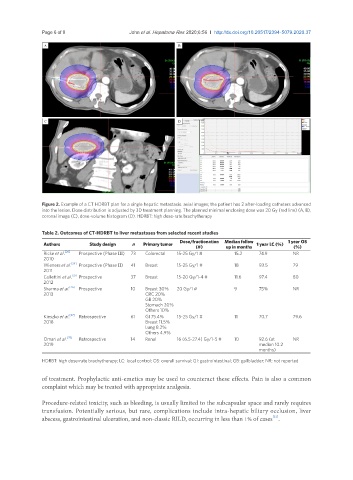
Figure 2. Example of a CT HDRBT plan for a single hepatic metastasis. axial images; the patient has 2 after-loading catheters advanced
into the lesion. Dose distribution is adjusted by 3D treatment planning. The planned minimal enclosing dose was 20 Gy (red line) (A, B),
coronal image (C), dose-volume histogram (D). HDRBT: high dose-rate brachytherapy
Table 2. Outcomes of CT-HDRBT to liver metastases from selected recent studies
Dose/fractionation Median follow 1 year OS
Authors Study design n Primary tumor 1 year LC (%)
(#) up in months (%)
Ricke et al. [20] Prospective (Phase III) 73 Colorectal 15-25 Gy/1 # 15.2 74.9 NR
2010
Wieners et al. [24] Prospective (Phase II) 41 Breast 15-25 Gy/1 # 18 93.5 79
2011
Collettini et al. [25] Prospective 37 Breast 15-20 Gy/1-4 # 11.6 97.4 80
2012
Sharma et al. [26] Prospective 10 Breast 30% 20 Gy/1 # 9 75% NR
2013 CRC 20%
GB 20%
Stomach 20%
Others 10%
Kieszko et al. [27] Retrospective 61 GI 75.4% 15-25 Gy/1 # 11 70.7 79.6
2018 Breast 11.5%
Lung 8.2%
Others 4.9%
Omari et al. [28] Retrospective 14 Renal 16 (6.5-27.4) Gy/1-5 # 10 92.6 (at NR
2019 median 10.2
months)
HDRBT: high dose-rate brachytherapy; LC: local control; OS: overall survival; GI: gastrointestinal; GB: gallbladder; NR: not reported
of treatment. Prophylactic anti-emetics may be used to counteract these effects. Pain is also a common
complaint which may be treated with appropriate analgesia.
Procedure-related toxicity, such as bleeding, is usually limited to the subcapsular space and rarely requires
transfusion. Potentially serious, but rare, complications include intra-hepatic biliary occlusion, liver
[21]
abscess, gastrointestinal ulceration, and non-classic RILD, occurring in less than 1% of cases .