
Page 292 - Read Online
P. 292
Butt et al. TAE for ruptured HCC in Pakistan
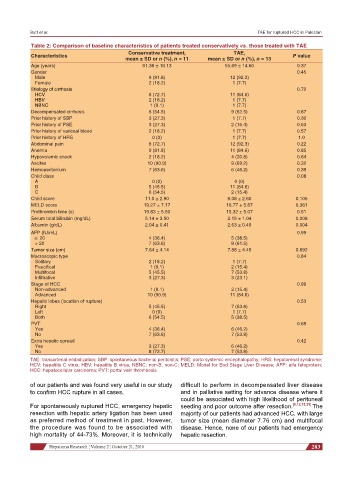
Table 2: Comparison of baseline characteristics of patients treated conservatively vs. those treated with TAE
Conservative treatment, TAE,
Characteristics P value
mean ± SD or n (%), n = 11 mean ± SD or n (%), n = 13
Age (years) 61.36 ± 16.13 55.69 ± 14.60 0.37
Gender 0.45
Male 9 (81.8) 12 (92.3)
Female 2 (18.2) 1 (7.7)
Etiology of cirrhosis 0.72
HCV 8 (72.7) 11 (84.6)
HBV 2 (18.2) 1 (7.7)
NBNC 1 (9.1) 1 (7.7)
Decompensated cirrhosis 6 (54.5) 9 (62.5) 0.67
Prior history of SBP 3 (27.3) 1 (7.7) 0.30
Prior history of PSE 3 (27.3) 2 (15.4) 0.63
Prior history of variceal bleed 2 (18.2) 1 (7.7) 0.57
Prior history of HRS 0 (0) 1 (7.7) 1.0
Abdominal pain 8 (72.7) 12 (92.3) 0.22
Anemia 9 (81.8) 11 (84.6) 0.85
Hypovolemic shock 2 (18.2) 4 (30.8) 0.64
Ascites 10 (90.9) 9 (69.2) 0.32
Hemoperitonium 7 (63.6) 6 (46.2) 0.39
Child class 0.08
A 0 (0) 0 (0)
B 5 (45.5) 11 (84.6)
C 6 (54.5) 2 (15.4)
Child score 11.0 ± 2.90 9.08 ± 2.60 0.105
MELD score 19.27 ± 7.17 16.77 ± 5.67 0.361
Prothrombin time (s) 19.83 ± 5.50 15.32 ± 5.07 0.51
Serum total bilirubin (mg/dL) 5.14 ± 3.50 2.15 ± 1.04 0.008
Albumin (g/dL) 2.04 ± 0.41 2.63 ± 0.49 0.004
AFP (IU/mL) 0.99
≤ 20 4 (36.4) 5 (38.5)
> 20 7 (63.6) 8 (61.5)
Tumor size (cm) 7.64 ± 4.14 7.88 ± 4.45 0.892
Macroscopic type 0.84
Solitary 2 (18.2) 1 (7.7)
Paucifical 1 (9.1) 2 (15.4)
Multifocal 5 (45.5) 7 (53.8)
Infiltrative 3 (27.3) 3 (23.1)
Stage of HCC 0.99
Non-advanced 1 (9.1) 2 (15.4)
Advanced 10 (90.9) 11 (84.6)
Hepatic lobes (location of rupture) 0.53
Right 5 (45.5) 7 (53.8)
Left 0 (0) 1 (7.7)
Both 6 (54.5) 5 (38.5)
PVT 0.69
Yes 4 (36.4) 6 (46.2)
No 7 (63.6) 7 (53.8)
Extra hepatic spread 0.42
Yes 3 (27.3) 6 (46.2)
No 8 (72.7) 7 (53.8)
TAE: transarterial embolization; SBP: spontaneous bacterial peritonitis; PSE: porto systemic encephalopathy; HRS: hepatorenal syndrome;
HCV: hepatitis C virus; HBV: hepatitis B virus; NBNC: non-B, non-C; MELD: Model for End Stage Liver Disease; AFP: alfa fetoprotein;
HCC: hepatocellular carcinoma; PVT: portal vein thrombosis
of our patients and was found very useful in our study difficult to perform in decompensated liver disease
to confirm HCC rupture in all cases. and in palliative setting for advance disease where it
could be associated with high likelihood of peritoneal
For spontaneously ruptured HCC, emergency hepatic seeding and poor outcome after resection. [6,12,18,25] The
resection with hepatic artery ligation has been used majority of our patients had advanced HCC, with large
as preferred method of treatment in past. However, tumor size (mean diameter 7.76 cm) and multifocal
the procedure was found to be associated with disease. Hence, none of our patients had emergency
high mortality of 44-73%. Moreover, it is technically hepatic resection.
Hepatoma Research ¦ Volume 2 ¦ October 21, 2016 283