
Page 56 - Read Online
P. 56
Page 12 of 15 Otsuka et al. Hepatoma Res 2021;7:5 I http://dx.doi.org/10.20517/2394-5079.2020.112
A B
C D
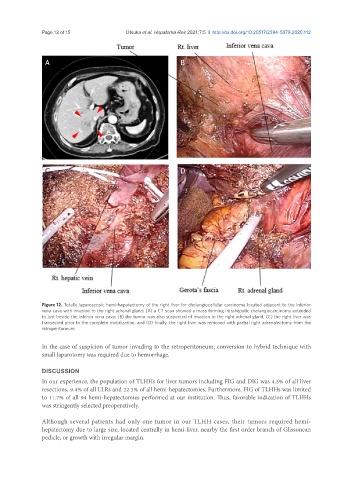
Figure 12. Totally laparoscopic hemi-hepatectomy of the right liver for cholangiocellular carcinoma located adjacent to the inferior
vena cava with invasion to the right adrenal gland: (A) a CT scan showed a mass forming intrahepatic cholangiocarcinoma extended
to just beside the inferior vena cava; (B) the tumor was also suspected of invasion to the right adrenal gland; (C) the right liver was
transected prior to the complete mobilization; and (D) finally, the right liver was removed with partial right adrenalectomy from the
retroperitoneum
In the case of suspicion of tumor invading to the retroperitoneum, conversion to hybrid technique with
small laparotomy was required due to hemorrhage.
DISCUSSION
In our experience, the population of TLHHs for liver tumors including FIG and DIG was 4.3% of all liver
resections, 9.4% of all LLRs and 22.3% of all hemi-hepatectomies. Furthermore, FIG of TLHHs was limited
to 11.7% of all 94 hemi-hepatectomies performed at our institution. Thus, favorable indication of TLHHs
was stringently selected preoperatively.
Although several patients had only one tumor in our TLHH cases, their tumors required hemi-
hepatectomy due to large size, located centrally in hemi-liver, nearby the first order branch of Glissonean
pedicle, or growth with irregular margin.