
Page 116 - Read Online
P. 116
Pegoraro et al. Hepatoma Res 2021;7:24 https://dx.doi.org/10.20517/2394-5079.2020.142 Page 7 of 12
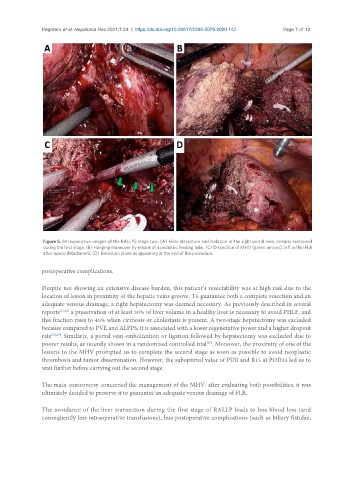
Figure 5. Intraoperative images of the RALLPS stage two. (A) Hilar dissection and isolation of the right portal vein, already sectioned
during the first stage. (B) Hanging maneuver by means of a pediatric feeding tube. (C) Dissection of MHV (green arrows), left within FLR
after tumor detachment. (D) Resection plane as appearing at the end of the procedure.
postoperative complications.
Despite not showing an extensive disease burden, this patient’s resectability was at high risk due to the
location of lesion in proximity of the hepatic veins groove. To guarantee both a complete resection and an
adequate venous drainage, a right hepatectomy was deemed necessary. As previously described in several
reports [21,22] a preservation of at least 30% of liver volume in a healthy liver is necessary to avoid PHLF, and
this fraction rises to 40% when cirrhosis or cholestasis is present. A two-stage hepatectomy was excluded
because compared to PVE and ALPPS, it is associated with a lower regenerative power and a higher dropout
rate [23,24] . Similarly, a portal vein embolization or ligation followed by hepatectomy was excluded due to
poorer results, as recently shown in a randomized controlled trial . Moreover, the proximity of one of the
[25]
lesions to the MHV prompted us to complete the second stage as soon as possible to avoid neoplastic
thrombosis and tumor dissemination. However, the suboptimal value of PDR and R15 at POD23 led us to
wait further before carrying out the second stage.
The main controversy concerned the management of the MHV: after evaluating both possibilities, it was
ultimately decided to preserve it to guarantee an adequate venous drainage of FLR.
The avoidance of the liver transection during the first stage of RALLP leads to less blood loss (and
consequently less intraoperative transfusions), less postoperative complications (such as biliary fistulae,