
Page 114 - Read Online
P. 114
Pegoraro et al. Hepatoma Res 2021;7:24 https://dx.doi.org/10.20517/2394-5079.2020.142 Page 5 of 12
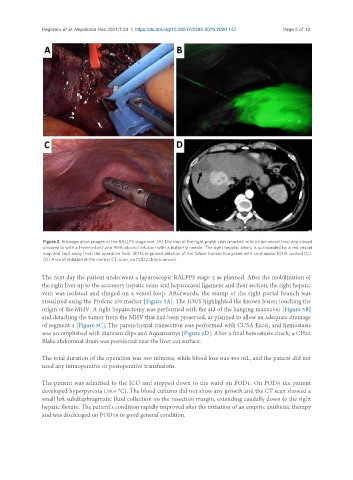
Figure 3. Intraoperative images of the RALLPS stage one. (A) Division of the right portal vein (marked with a blue vessel loop and closed
proximally with a Hem-o-Lok) and 96% alcohol infusion with a butterfly needle. The right hepatic artery is surrounded by a red vessel
loop and kept away from the operative field. (B) ICG-guided ablation of the future transection plane with continuous IOUS control (C).
(D) Area of ablation at the control CT-scan, on POD2 (black arrow).
The next day the patient underwent a laparoscopic RALPPS stage-2 as planned. After the mobilization of
the right liver up to the accessory hepatic veins and hepatocaval ligament and their section, the right hepatic
vein was isolated and slinged on a vessel loop. Afterwards, the stump of the right portal branch was
visualized using the Prolene 2/0 marker [Figure 5A]. The IOUS highlighted the known lesion touching the
origin of the MHV. A right hepatectomy was performed with the aid of the hanging maneuver [Figure 5B]
and detaching the tumor from the MHV that had been preserved, as planned to allow an adequate drainage
of segment 4 [Figure 5C]. The parenchymal transection was performed with CUSA Excel, and hemostasis
was accomplished with titanium clips and Aquamantys [Figure 5D]. After a final hemostasis check, a CH24
Blake abdominal drain was positioned near the liver cut surface.
The total duration of the operation was 360 minutes, while blood loss was 400 mL, and the patient did not
need any intraoperative or postoperative transfusions.
The patient was admitted to the ICU and stepped down to the ward on POD1. On POD5 the patient
developed hyperpyrexia (38.4 °C). The blood cultures did not show any growth and the CT scan showed a
small left subdiaphragmatic fluid collection on the resection margin, extending caudally down to the right
hepatic flexure. The patient’s condition rapidly improved after the initiation of an empiric antibiotic therapy
and was discharged on POD16 in good general condition.