
Page 115 - Read Online
P. 115
Page 6 of 12 Pegoraro et al. Hepatoma Res 2021;7:24 https://dx.doi.org/10.20517/2394-5079.2020.142
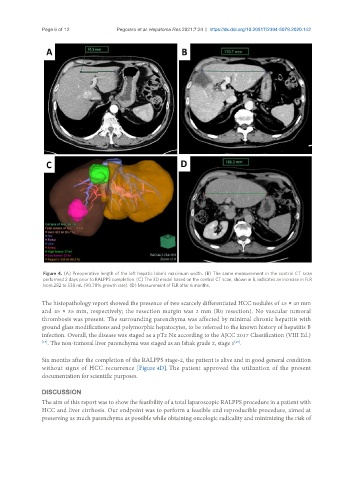
Figure 4. (A) Preoperative length of the left hepatic lobe’s maximum width. (B) The same measurement in the control CT scan
performed 2 days prior to RALPPS completion. (C) The 3D model based on the control CT scan, shown in B, indicates an increase in FLR
from 282 to 538 mL (90.78% growth rate). (D) Measurement of FLR after 6 months.
The histopathology report showed the presence of two scarcely differentiated HCC nodules of 45 × 40 mm
and 45 × 35 mm, respectively; the resection margin was 2 mm (R0 resection). No vascular tumoral
thrombosis was present. The surrounding parenchyma was affected by minimal chronic hepatitis with
ground glass modifications and polymorphic hepatocytes, to be referred to the known history of hepatitis B
infection. Overall, the disease was staged as a pT2 Nx according to the AJCC 2017 Classification (VIII Ed.)
[19] . The non-tumoral liver parenchyma was staged as an Ishak grade 2, stage 1 .
[20]
Six months after the completion of the RALPPS stage-2, the patient is alive and in good general condition
without signs of HCC recurrence [Figure 4D]. The patient approved the utilization of the present
documentation for scientific purposes.
DISCUSSION
The aim of this report was to show the feasibility of a total laparoscopic RALPPS procedure in a patient with
HCC and liver cirrhosis. Our endpoint was to perform a feasible and reproducible procedure, aimed at
preserving as much parenchyma as possible while obtaining oncologic radicality and minimizing the risk of